A Work in Progress





Most hospitalist programs start when hospital administrators realize that having physicians dedicated exclusively to inpatient care is a great idea. Administrators then recruit a lead hospitalist—perhaps a stellar performer straight from residency, a community doctor closing his office, or a doctor located through a specialty staffing group.
Colorado Permanente Medical Group (CPMG), backed by a brand as powerful as Starbucks or Nordstrom, did things differently. So imbued with the Permanente culture are its physicians that its hospitalist group arose organically from physicians serving Denver’s Exempla St. Joseph Hospital and Boulder Community Hospital. (See “Kaiser Permanente Culture,” below.)
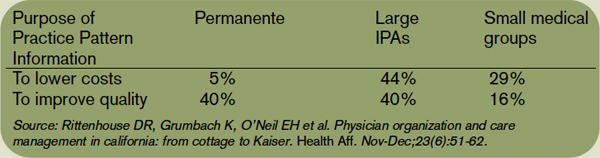
It found that Permanente physicians value quality-oriented, system-level care management tools to a much greater degree than other physicians. In the study, 22% of primary care physicians in California practiced with Permanente, 16% with other groups of 11 or more physicians, 44% were in groups of one to 10 and participated in at least one Independent Practice Association (IPA), and 18% represented the “cottage industry” sector-solo or small groups with no IPA participation.
Sixty percent of Permanente physicians received practice pattern information, while less than 25% of cottage industry doctors did. Almost all Permanente primary care physicians (PCPs) who received such information described it as very or somewhat useful, versus 79% of PCPs in other groups.
The PCPs revealed their mindset in questions about cost versus quality.
The authors concluded that “Physicians in large, integrated Permanente medical groups have adopted and used value system-level care management tools, much more so than physicians in IPA settings or traditional cottage-industry practices.”—MP
“Thirty years ago Permanente explored building their own versus finding a cost-effective hospital. They chose us, and their clinic doctors rounded on what grew to 70% of our department of medicine patients,” says Robert Gibbons, MD, St. Joseph’s residency program director. “Then they saw they needed to provide full-time inpatient coverage—the advent of the hospitalist program. Soon many CPMG clinic doctors disappeared, but the quality of medicine remained the same.”
Regional Department Chief Lauren Fraser, MD, oversees the now-mature hospitalist program, which keeps growing in size, complexity, and competence. “We’re always a work in progress, and that’s good,” she says.
According to Joe Heaton, MD, currently a Good Samaritan hospitalist and formerly CPMG regional department chief, CPMG’s primary care departments targeted three areas for better care early in 1995: streamlining patient scheduling, developing a centralized call center, and starting a hospitalist program.
The hospitalist program aimed for cost neutrality by limiting staffing at both hospitals to the same full-time equivalents (FTEs). To avoid forcing physicians into unwelcome assignments, the department offered its 70 internal medicine and 30 family practice doctors four tracks:
- Track A meant full-time hospital work;
- Track B offered a 50-50 hospital-clinic split;
- Track C provided for a 70% clinic, 30% hospital schedule; and
- Track D was full-time clinic work.
The family medicine department opted out of hospital duty, while the internists tracked themselves as follows: eight each for full-time hospital and half-time hospital duty, 34 for 30% hospital time, and 20 for full-time clinic. Fortunately, the tracks chosen matched the hospitals’ needs, and the program was off and running by July 1995.
“At the time, our group’s size created one of the largest hospitalist programs, allowing us to provide 24/7 coverage with at least two physicians on site,” says Dr. Heaton of the launch.