In the era of duty hour regulations, there is increasing concern regarding resident workload compression. We conducted a retrospective, observational assessment of all internal medicine resident admissions to a Veterans Affairs hospital over a 15-year period to evaluate several admission components that impact resident workload and workload intensity, including electronic health record (EHR) data burden and patient comorbidity. A total of 67,346 admissions were included in the analysis. Mean patient comorbidity, as measured by the Charlson Comorbidity Index, increased throughout the study period. EHR data burden, measured by numbers of notes, medications, and discharge summaries available per patient at the time of admission, also increased over the study period. These findings suggest that EHR data burden and comorbidity have increased over time, which impacts resident workload in the era of duty hour restrictions.
© 2018 Society of Hospital Medicine
Since the Accreditation Council for Graduate Medical Education (ACGME) posed new duty hour regulations in 2003 and again in 2011, there have been concerns that the substantial compression of resident workload may have resulted in a negative learning environment.1-3 Residents are now expected to complete more work in a reduced amount of time and with less flexibility.4 In addition to time constraints, the actual work of a resident today may differ from that of a resident in the past, especially in the area of clinical documentation.5 Restricting resident work hours without examining the workload may result in increased work intensity and counter the potential benefits of working fewer hours.6 Measuring workload, as well as electronic health record (EHR)–related stress, may also help combat burnout in internal medicine.7 There are many components that influence resident workload, including patient census, patient comorbidities and acuity,EHR data and other available documentation, and ancillary tasks and procedures.7 We define resident workload intensity as the responsibilities required to provide patient care within a specified time. There is a paucity of objective data regarding the workload intensity of residents, which are essential to graduate medical education reform and optimization. Patient census, ancillary responsibilities, number of procedures, and conference length and frequency are some of the variables that can be adjusted by each residency program. As a first step to objective measurement of resident workload intensity, we endeavored to evaluate the less easily residency program–controlled workload components of patient comorbidity and EHR data the time of patient admission.
We conducted an observational, retrospective assessment of all admissions to the Louis Stokes Cleveland VA Medical Center (LSCVAMC) internal medicine service from January 1, 2000 to December 31, 2015. The inclusion criteria were admission to non-ICU internal medicine services and an admission note written by a resident physician. Otherwise, there were no exclusions. Data were accessed using VA Informatics and Computing Infrastructure. This study was approved by the LSCVAMC institutional review board.
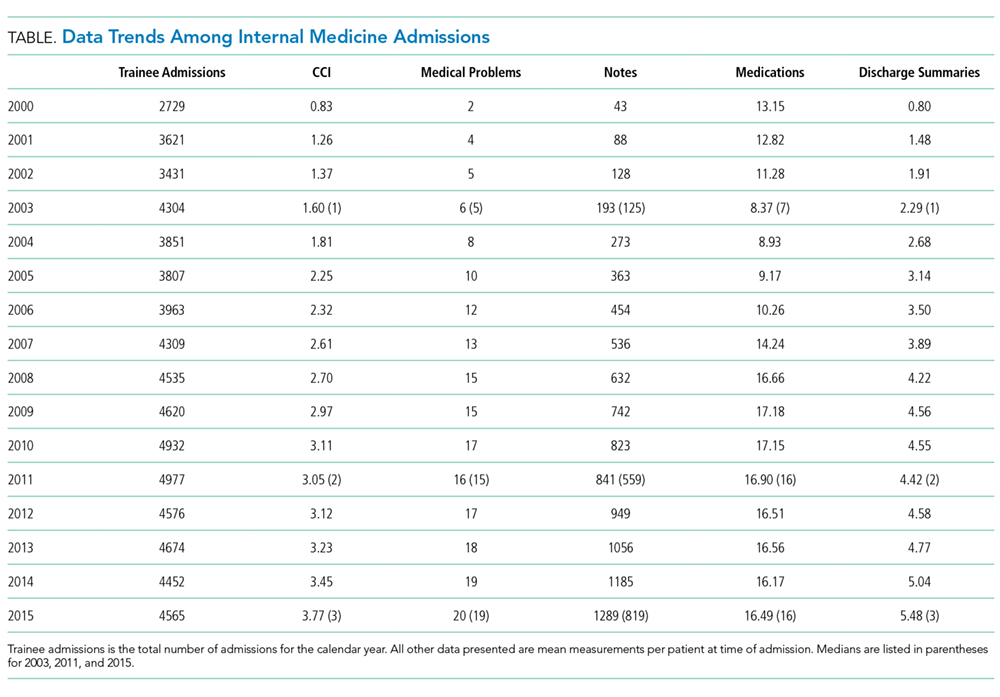
We evaluated multiple patient characteristics for each admission that were accessible in the EHR at the time of hospital admission including patient comorbidities, medication count, and number of notes and discharge summaries. The Charlson Comorbidity Index (CCI) Deyo version was used to score all patients based on the EHR’s active problem list at the time of admission.8,9 The CCI is a validated score created by categorizing comorbidities using International Classification of Diseases, Ninth and Tenth Revisions.8 Higher CCI scores predict increased mortality and resource usage. For each admission, we also counted the number of active medications, the number of prior discharge summaries, and the total number of notes available in the EHR at the time of patient admission. Patient admissions were grouped by calendar year, the mean numbers of active medications, prior discharge summaries, and total available notes per patient during each year were calculated (Table). Data comparisons were completed between 2003 and 2011 as well as between 2011 and 2015; median data are also provided for these years (Table). These years were chosen based on the years of the duty hour changes as well as comparing a not brand new, but still immature EHR (2003), a mature EHR (2011), and the most recent available data (2015).
A total of 67,346 admissions were included in the analysis. All parameters increased from 2000 to 2015. Mean CCI increased from 1.60 in 2003 (95% CI, 1.54–1.65) to 3.05 in 2011 (95% CI, 2.97–3.13) and to 3.77 in 2015 (95% CI, 3.67–3.87). Mean number of comorbidities increased from 6.21 in 2003 (95% CI, 6.05–6.36) to 16.09 in 2011 (95% CI, 15.84–16.34) and to 19.89 in 2015 (95% CI, 19.57–20.21). Mean number of notes increased from 193 in 2003 (95% CI, 186–199) to 841 in 2011 (95% CI, 815–868) and to 1289 in 2015 (95% CI, 1243–1335). Mean number of medications increased from 8.37 in 2003 (95% CI, 8.15–8.59) to 16.89 in 2011 (95% CI 16.60–17.20) and decreased to 16.49 in 2015 (95% CI, 16.18–16.80). Mean number of discharge summaries available at admission increased from 2.29 in 2003 (95% CI, 2.19–2.38) to 4.42 in 2011 (95% CI, 4.27–4.58) and to 5.48 in 2015 (95% CI, 5.27–5.69).