Hospital Perceptions of Medicare’s Sepsis Quality Reporting Initiative





BACKGROUND: In October 2015, the Centers for Medicare and Medicaid Services (CMS) implemented the Sepsis CMS Core Measure (SEP-1) program, requiring hospitals to report data on the quality of care for their patients with sepsis.
OBJECTIVE: We sought to understand hospital perceptions of and responses to the SEP-1 program.
DESIGN: A thematic content analysis of semistructured interviews with hospital quality officials.
SETTING: A stratified random sample of short-stay, nonfederal, general acute care hospitals in the United States.
SUBJECTS: Hospital quality officers, including nurses and physicians.
INTERVENTION: None.
MEASUREMENTS: We completed 29 interviews before reaching content saturation.
RESULTS: Hospitals reported a variety of actions in response to SEP-1, including new efforts to collect data, improve sepsis diagnosis and treatment, and manage clinicians’ attitudes toward SEP-1. These efforts frequently required dedicated resources to meet the program’s requirements for treatment and documentation, which were thought to be complex and not consistently linked to patient-centered outcomes. Most respondents felt that SEP-1 was likely to improve sepsis outcomes. At the same time, they described specific changes that could improve its effectiveness, including allowing hospitals to focus on the treatment processes most directly associated with improved patient outcomes and better aligning the measure’s sepsis definitions with current clinical definitions.
CONCLUSIONS: Hospitals are responding to the SEP-1 program across a number of domains and in ways that consistently require dedicated resources. Hospitals are interested in further revisions to the program to alleviate the burden of the reporting requirements and help them optimize the effectiveness of their investments in quality-improvement efforts.
© 2017 Society of Hospital Medicine
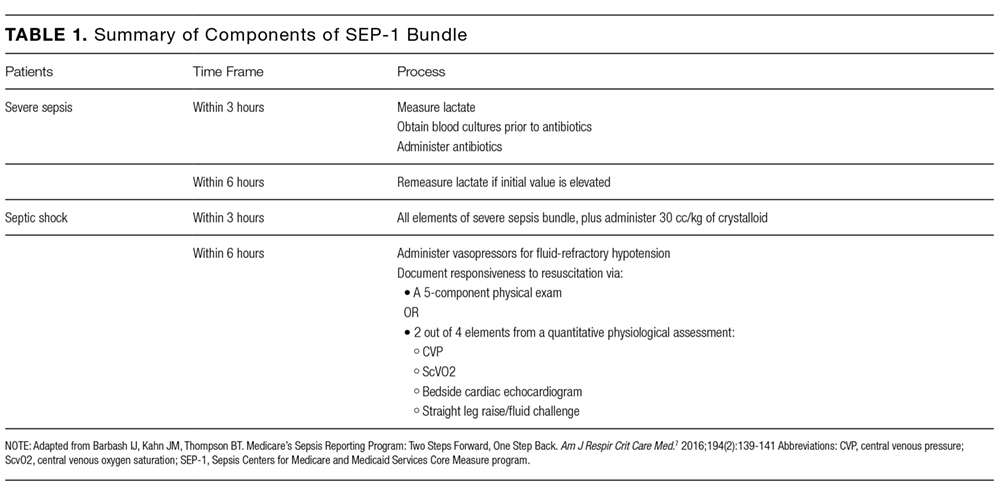
Sepsis affects over 1 million Americans annually, resulting in significant morbidity, mortality, and costs for hospitalized patients.1-4 There is an increasing interest in policy-oriented approaches to improving sepsis care at both the state and national levels.5,6 The most prominent policy is the Centers for Medicare and Medicaid Services (CMS) Sepsis CMS Core (SEP-1) program, which was formally implemented in October 2015; the program mandates that hospitals report their compliance with a variety of sepsis treatment processes (Table 1). Academic quality experts generally applaud the increased attention to sepsis but are concerned that the measure’s design and specifications advance beyond the existing evidence base.7,8 However, remarkably little is known about how front-line hospital quality officials perceive the program and how they are responding or not responding, to the new requirements. This knowledge gap is a critical barrier to evaluating the program’s practical impact on sepsis treatment and outcomes.
METHODS
Study Design, Setting, and Subjects
We conducted a qualitative study by using semistructured telephone interviews with hospital quality officers in the United States. We targeted hospital quality officers because they are in a position to provide overarching insights into hospitals’ perceptions of and responses to the SEP-1 program. We enrolled quality officers at general, short-stay, nonfederal acute care hospitals because those are the hospitals to which the SEP-1 program applies. We generated a stratified random sample of hospitals by using 2013 data from Medicare’s Healthcare Cost and Reporting Information System (HCRIS) database.10 We stratified by size (greater than or less than 200 total beds), teaching status (presence or absence of any resident physician trainees), and ownership (for-profit vs nonprofit), creating 8 mutually exclusive strata. This sampling frame was designed to ensure representativeness from a broad range of hospital types, not to enable comparisons across hospital types, which is outside the scope of qualitative research.
Within strata, we contacted hospitals in a random order by phone using the primary number listed in the HCRIS database. We asked the hospital operator to connect us to the chief quality officer or an appropriate alternative hospital administrator with knowledge of hospital quality-improvement activities. We limited participation to 1 respondent per hospital. We did not offer any specific incentives for participation.
The study was approved by the University of Pittsburgh Institutional Review Board with a waiver of signed informed consent.
Data Collection
Interviews were conducted by a trained research coordinator between February 2016 and October 2016. Interviews were conducted concurrently with data analysis by using a constant comparison approach.11 The constant comparison approach involves the iterative refinement of themes by comparing the existing themes to new data as they emerge during successive interviews. We chose a constant comparison approach because we wanted to systematically describe hospital responses to SEP-1 rather than specifically test individual hypotheses.11 As is typical in qualitative research, we did not set the sample size a priori but instead continued the interviews until we achieved thematic saturation.12,13
The interview script included a mix of directed and open-ended questions about respondents’ perspectives of and hospital responses to the SEP-1 program. The questions covered the following 4 domains: hospitals’ sepsis quality-improvement initiatives before and after the Medicare reporting program, reception of the hospital responses, the approach to data abstraction and reporting, and the overall impressions of the program and its impact.6-8,14 We allowed for updates and revisions of the interview guide as necessary to explore any new content and emergent themes. We piloted the interview guide on 2 hospital quality officers at our institution and then revised its structure again after interviews with the initial 6 hospitals. The complete final interview guide is available in the supplemental digital content.