
Perioperative care of the elderly patient: An update*





ABSTRACT
Elderly patients pose unique challenges perioperatively. They are more likely than younger surgical patients to be mentally and physically compromised at baseline, which increases the risk of delirium and postoperative cognitive dysfunction. Postoperative cognitive risk can be predicted, however, and effective strategies exist to reduce this risk. Elderly patients are also at increased risk of a precipitous postoperative decline in physiologic reserve, which can lead to organ failure. General recommendations for the perioperative care of elderly patients include avoiding drugs that raise the risk of delirium, ensuring adequate caloric and fluid intake, getting the patient out of bed and into physical therapy as soon as possible, and early planning for discharge. An elderly patient’s postoperative cognitive risk and its impact on quality of life should be factored into the decision whether to undergo surgery. Family conferences are recommended to address the many questions and challenges that surgery in an elderly person can pose.
KEY POINTS
- Postoperative cognitive dysfunction and delirium are distinct conditions, though both are common in the elderly. Postoperative cognitive dysfunction may persist for weeks to months and may not be obvious, whereas delirium, a disorder of attention and cognition, is easier to detect clinically.
- Major predictors of postoperative delirium are severe illness, baseline dementia, dehydration, and sensory impairment.
- Drugs that raise dementia risk include anticholinergics, benzodiazepines, meperidine, tricyclic antidepressants, first-generation antihistamines, and high-dose H2-receptor blockers.
- Early performance of hip fracture surgery in the elderly (ie, within 24 hours of admission) has not been shown to lower mortality but appears to improve other outcomes.
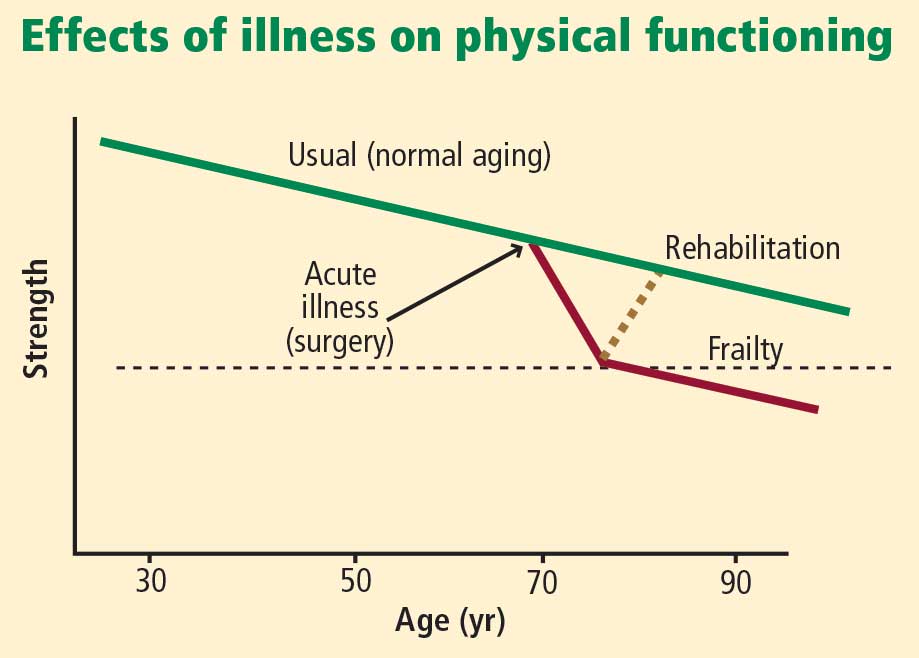
- Identifying and managing frail elderly patients is important. Signs of frailty are minimal activity, generalized muscle weakness, slowed performance, fatigue, and weight loss.
Frailty is important to recognize
It is important to identify frailty and to aggressively manage frail patients postoperatively. Although frailty is not clearly defined, Fried et al17 identified five clinical features that correlate with its underlying pathophysiology:
- Minimal physical activity (ie, “doing less”)
- Generalized (not focal) muscle weakness
- Slowed performance (eg, walking short distances takes longer)
- Fatigue or poor endurance
- Unintentional weight loss.
The presence of three or more of these features meets the criteria for frailty and is associated with increased risk for mortality over the next 3 years with or without surgery,17 although surgery probably increases the risk.
Frailty is believed to be a failure over time of the homeostatic mechanisms that keep our organ systems functioning in the face of a stress. Decline in the ability of organ systems to maintain normal function is probably caused by inflammation, chronic disease, and normal aging, and has been termed homeostenosis. As a person ages and physiologic reserves are reduced, adding a stress such as surgery or severe infection can result in organ failure—usually multiple-system organ failure. In any intensive care unit, one is likely to see elderly patients who were admitted with one medical or surgical problem and soon end up having renal, liver, or brain dysfunction as well.
Physical therapy immediately after hip fracture surgery is associated with significantly better locomotion 2 months later.18 A number of exercises are effective: range-of-motion exercises, low-impact aerobic activities, and exercises starting with low-intensity resistance (using bands, tubes, and weights) and progressing as tolerated to high-intensity resistance (with machines and pulleys) for an extended period of time.
Nutrition supplementation
Malnourishment can contribute to frailty, yet evidence for the benefits of supplementing nutrition is not strong, as noted above. However, meta-analyses of studies of nutritional interventions with meal supplementation (usually canned supplements) show that meal supplementation can improve mortality risk and reduce morbidity such as pressure ulcers in hospitalized elderly patients.19,20 The patients most likely to benefit are those who are undernourished at baseline and aged 75 years or older.
CASE CONTINUED: WHAT HAPPENS POST-DISCHARGE?
Following surgery, our patient wonders, “Where will I go next? What will my lifestyle be like?”
These are important questions to consider when first evaluating whether an elderly patient should undergo surgery. In the case of hip fracture, standard thinking is that without surgery, the patient will never recover the ability to independently walk and perform activities of daily living. But we also must recognize the considerable risks of surgery in the elderly population, particularly those aged 75 years or older.
Comprehensive discharge planning
Early and intensive discharge management enhances quality of life and may help reduce hospital costs. A good model of care involves collaboration of orthopedic surgeons, hospitalists, general internists, geriatricians, and dietitians to address procedures, diet and nutrition, mobility and activities of daily living, and pain medications.21 A case manager such as a social worker should start addressing care transition the day after surgery—planning ahead is imperative.
Following hip surgery, patients are routinely sent to skilled nursing facilities as soon as possible so they can start intensive physical therapy. Patients with significant functional impairment or who had delirium are more likely to require a prolonged hospital stay.
Naylor et al examined the effectiveness of comprehensive discharge planning in a study that randomized hospitalized patients (including surgical patients) 65 years or older to either usual discharge planning or intensive discharge planning with advanced practice nurses beginning early in hospitalization.22 The intervention group was followed by home care nurses for up to 4 weeks and had continuous telephone access to the nurses. Patients who received the intervention had a significantly lower risk of hospital readmission, and those who were readmitted had significantly shorter hospital stays. The total cost of care was also significantly lower in the intervention group.
Family conferences aid decision making
Family conferences can be very useful for working through the many questions and challenges that surgery in an elderly person can pose, including whether the patient should undergo the operation, postoperative management, and postdischarge placement.23 For patients with an uncertain prognosis because of unclear or multiple concurrent diseases, a family conference can help clarify the goals of therapy, inform the family about likely outcomes, and help determine the patient’s wishes and values. Such issues should be revisited as the postoperative course proceeds.
Family conferences also provide a good opportunity to review advanced directives, the need for life support, and possible transfers to intensive care. Family conferences can also help resolve conflicts in care management, as family members may not agree with the need for surgery, how aggressive treatment should be, or where to send the patient for rehabilitation. Differences among family members on these questions are especially common with elderly patients. Working out such issues will improve patient care, especially when done early in the hospitalization.
