Psychological Stress Interventions and Asthma: Therapeutic Considerations





From the Department of Medicine, The University of Mississippi Medical Center, Jackson, MS.
Abstract
- Objective: To review psychological stress interventions employed to improve asthma outcomes.
- Methods: Review of the literature.
- Results: In general, there are 2 approaches to managing stress in asthma patients—direct psychological interventions, and modalities where stress management is an indirect effect. The most direct approach involves mindfulness-based stress reduction, which has been shown to have a positive effect on asthma control. Cognitive behavioral therapy, biofeedback, music therapy, art therapy, and relaxation training also have been evaluated with varying results. Physical therapies, including yoga, chi gong, massage, reflexology, specific controlled breathing programs, and spinal manipulation have also been studied without consistent effectiveness demonstrated. Pharmacologic therapy for anxiety and depressive disorders has been shown to be associated with improvement in asthma symptoms and control.
- Conclusion: Although further research is needed to verify the beneficial role of specific stress intervention modalities for specific asthma populations, there is sufficient evidence of efficacy to validate the concept of stress management as a viable therapeutic approach for optimal asthma control.
The increasing levels of chronic psychological stress in the people’s everyday lives has been well recognized [1]. As technological advances continue to progress, the psychological and physical pressures associated with family- and work-role expectations, decreased free or “down” time, greater sleep deficits, increasing career-related pressures, social issues, and other factors have led to ever increasing levels of personal stress [2]. From an immune standpoint, these chronic stressors impact immune balance and may be at least partially responsible for the rise in incidence, prevalence, and severity of inflammatory diseases such as asthma [3]. As the factors responsible for increased levels of psychosocial stress in our society are not likely to decrease in the near future [4], the potential value of directed stress intervention therapies in the overall care plans for patients with asthma is an area of interest. Such stress management strategies must be evidence-based, pragmatic, and cost-effective. This review provides background, scientific and clinical rationale, and progress to date for various therapeutic approaches to stress management for asthma patients.
Asthma as Inflammatory Disease
Asthma is a breathlessness syndrome typically characterized by varying combinations of paroxysmal wheezing, cough, breathlessness, and chest tightness. The constellation of symptoms is often precipitated by exposure to volatile irritants, allergens, cold air, and exercise. Gastroesophageal reflux disease, respiratory viral infections, and pregnancy may also precipitate or worsen existing asthma [5,6]. Symptoms typically improve after appropriate asthma treatment.
While the role of IgE-mediated mechanisms in asthma has been questioned by some, studies have demonstrated the presence of IgE-mediated (“allergic”) mechanisms in most asthma cases [7]. Depending on the specific population, as many as 70% to 90% of asthma patients can be considered to have an allergic component to their asthma [8]. Such allergic sensitivities can be to seasonal pollens but even more commonly to perennial allergens such as dust mites, molds, cockroaches, and pet dander (especially cat) [9]. These associations have led to therapeutic approaches for many asthma patients based largely on those classically used for allergic rhinitis, including avoidance, environmental control, and even allergen immunotherapy [10]. Some of the newest and most promising pharmacotherapies for asthma are based on antagonism and/or prevention of the allergic cascade (production and activity of IgE) [11].
Psychological Stress and Asthma
Research regarding the relationships between asthma and chronic stress has been conducted in a variety of populations, using both cross-sectional and prospective designs [12,13]. It has been found that perceived stress negatively affects quality of life of patients with asthma and is associated with reduced medication compliance [14,15] and symptom perception [14,16]. Stress has been linked to both the onset of allergic asthma [17,18] and to enhanced skin test reactivity in response to allergens [19].Oh et al [12] suggested a dose-dependent relationship, with individuals who report increasingly higher levels of stress being more likely to report symptoms of asthma.
People with asthma who are exposed to various types of chronic stress tend to have worse severity and poorer control of their asthma symptoms [20,21]. Interventions to help manage stress in people with asthma are needed at the individual, family, and community levels; all levels are known to influence asthma and asthma morbidity [20,22].
If stress is associated with increased disease incidence and severity, then stress modulation could be expected to have beneficial effects. Advice to work fewer hours, get more sleep, and optimize relaxation can be unproductive and even frustrating to busy persons striving to meet all the demands of life. More realistic are interventions based upon helping people manage stress. Studies have reported benefit from stress management for a number of chronic diseases, including hypertension [23], obesity [24], diabetes [25], and HIV [26]. Given the associations noted above, stress intervention as a therapeutic modality for asthma management is a valid option that should be explored [27].
Psychologically Focused Interventions
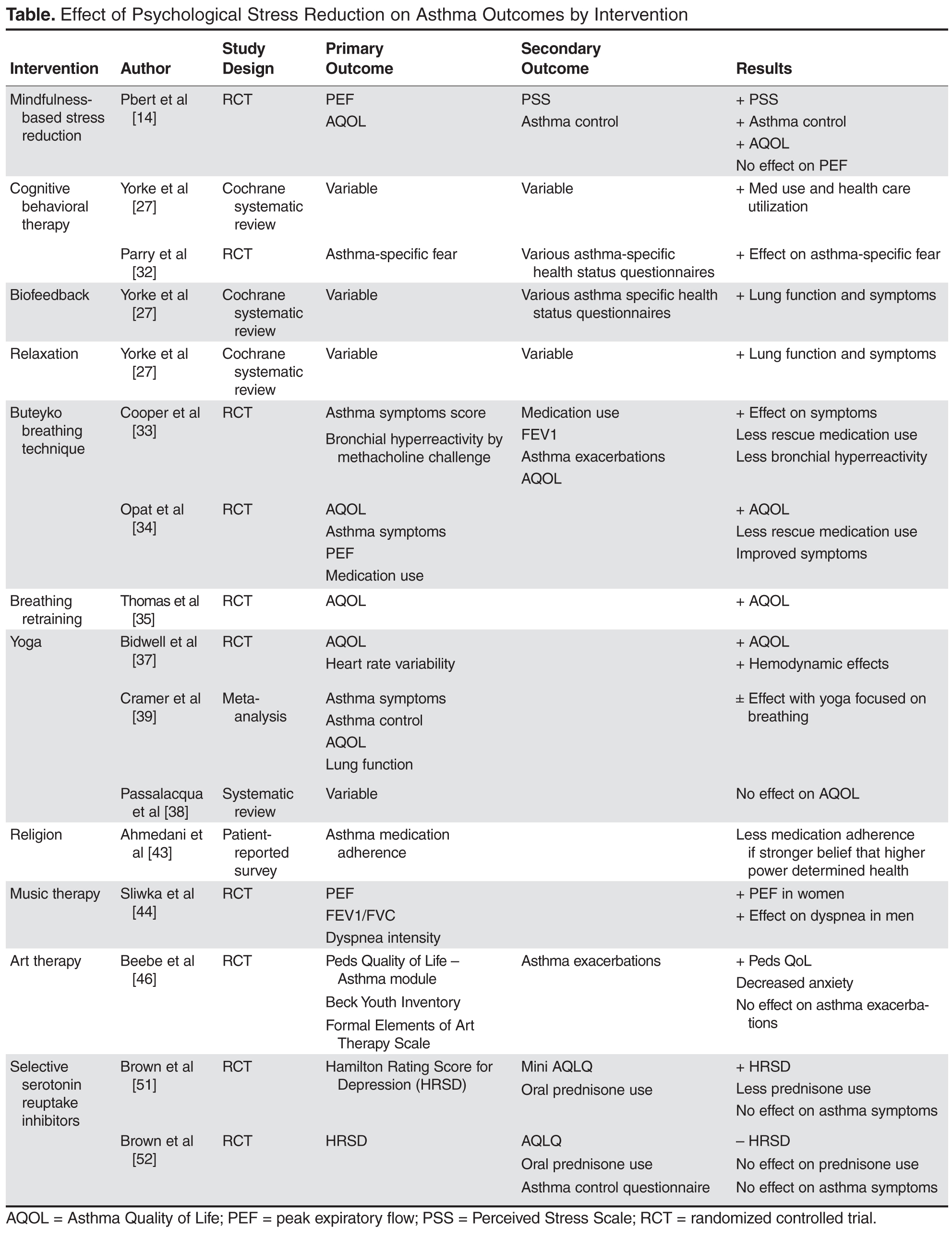
Mindfulness-based stress reduction (MBSR) has been recognized as an important modality for treatment of many chronic diseases, including chronic pain [28], cardiovascular disease [29], type 2 diabetes mellitus [29], cancer [30], and fibromyalgia [28]. MBSR teaches patients to recognize disease symptoms and personal reactions to these symptoms, and to develop a nonreactive awareness of these elements [14]. It is an individual or group-based therapeutic approach that uses education, discussion, and various meditation techniques to reduce perceived general and disease-associated stress [14,31]. Pbert et al performed an RCT comparing a MBSR program with a traditional education program in adults with mild, moderate, or severe persistent asthma. The primary outcomes were centered on lung function as measured by peak expiratory flow (PEF) and quality of life using the Asthma Quality of Life Questionnaire (AQLQ). Secondary outcomes included changes in perceived stress as measured by the 10-question Perceived Stress Scale (PSS) and overall asthma control. At 12 months, results indicated that MBSR had positive effects on overall asthma control, with improvement in quality of life, a decrease in perceived stress, and a decrease in use of rescue therapies, but no significant effect on peak expiratory flow [14].
Various other psychological interventions have been studied as supplemental therapy to medications in the treatment of asthma. Yorke et al performed a systematic review of 14 RCTs evaluating various psychological interventions in asthma, including cognitive behavioral therapy (CBT), biofeedback, and various relaxation techniques [27]. Because there are no standardized outcomes measured across all studies, results are often conflicting. While CBT had a positive effect on asthma health care utilization, relaxation therapy had no significant effects; both did have positive effects on symptoms of depression and anxiety. Relaxation therapy had positive effects on relieving asthma symptoms such as cough and wheeze but CBT did not. Biofeedback and relaxation were the only interventions that had positive effect on improving lung function and decreasing medication usage [27].
In an RCT, Parry and colleagues evaluated the effects of CBT added to clinical care on asthma-specific fear when compared to standard clinical asthma care alone. They demonstrated a significant reduction in panic and fear related to asthma exacerbations using CBT [32].
Various other mind-body–based interventions, including meditation, yoga, and breathing techniques, have been evaluated as complementary asthma therapy. Several studies utilized the Buteyko breathing technique (BBT), which focuses on controlling breathing to restore normal levels of PaCo2 in order to improve tissue oxygenation and reduce bronchospasm. Cooper et al performed an RCT that evaluated asthma symptom scores and methacholine sensitivity (concentration of bronchial irritant causing decline in FEV1 > 20%) for the presence of bronchial hyperreactivity (BHR), a measure of asthma activity. The BBT group demonstrated a reduction in asthma symptoms and rescue inhaler use but no change in BHR [33]. Opat measured asthma QOL, asthma symptoms, rescue medication use, and lung function in patients who received instruction in BBT and patients in a sham control group. BBT was associated with improvement in asthma QOL and bronchodilator use but not in other outcome parameters [34]. Thomas et al demonstrated in an RCT involving asthma patients with symptoms of dysfunctional breathing that rebreathing-retraining physiotherapy improved asthma-related QOL compared with traditional nurse-provided education [35].
Physical Stress Management Interventions
Yoga, which involves various aspects of controlled breathing, stretching, and meditation techniques [36], aims to achieve synergy between the mind and body to produce a more relaxed psychophysiological state [37]. This popular modality is frequently used by patients, including those with asthma, for symptom control and disease management. Results from RCTs have varied in their reports of efficacy. The 2006 Allergic Rhinitis and Asthma (ARIA) work group performed a systematic review of 5 trials evaluating yoga and asthma. Though the quality of the trials varied greatly, the review demonstrated a possible benefit of yoga on asthma-related QOL but no other studied parameters [38]. QOL and hemodynamic improvement was also demonstrated in 1 RCT comparing yoga added to standard asthma therapy vs. standard therapy alone in female patients [37]. Cramer et al performed an extensive systematic review and meta-analysis of 14 RCTs evaluating the effects of yoga on all or some components of asthma-related QOL, asthma control, symptoms, and pulmonary function [39]. Though there may be some benefit of yoga breathing techniques on asthma-related QOL, the quality of these studies is very poor and reported results were highly variable. These limitations demonstrate the need for methodologically sound, standardized approaches to research in this field, which will be needed before definitive conclusions or treatment recommendations can be made [38,39].
Complementary and Alternative Medicine Interventions
Therapeutic massage, reflexology, spinal manipulation, and prayer are commonly used components of complementary medicine that are perceived by many to be helpful in asthma management [40,41]. However, the published data supporting these techniques is limited. In 2005, Hondras et al performed a Cochrane database review of RCTs evaluating manual therapy, including therapeutic massage, in asthma. Variations in measured outcomes, study design, and reporting made the evidence presented in the review difficult to interpret. Methodologically sound RCTs are needed before any inferences as to relative efficacy of these techniques can be drawn [42]. Since 2005, there have been no significant RCTs reported that would change this conclusion. Data on prayer, religious beliefs, and how these affect asthma and stress control are scarce. One nonrandomized patient reporting survey analysis to evaluate the presence of a high power in life and asthma medication adherence was reported by Ahmedani and colleagues. Results showed that overall medication adherence was low, particularly among those who believed a higher power was in control of their health [43].
Other relaxation methods for managing stress in asthma include music therapy [44] and art therapy [45,46]. Music therapy has had varying reported therapeutic success in other medical settings, such as cardiac rehabilitation [47] and prior to endoscopy [48]. Several studies have evaluated passive or active music therapy in various stages of asthma management with variable results reported. One RCT of patients admitted for asthma exacerbation evaluated the effectiveness of standard pulmonary rehabilitation for asthma with or without concomitant music therapy. Measured outcomes included lung function parameters (PEF and FEV1/FVC) and self-reported anxiety scales. There was a small improvement in PEF in women in the music therapy group. Secondary statistical analysis showed lung function improvements with music therapy only in the patients with mild asthma [44]. Art therapy, the opportunity to share feelings through the use of art materials and expressions, has been used effectively to reduce psychological distress in pediatric chronic disease. One RCT of 23 children examined the potential utility of art therapy in pediatric asthma management. While it did not affect number of exacerbations, art therapy dramatically improved quality of life in children with asthma by decreasing worry and anxiety. The effect persisted for at least 6 months after the intervention was completed [46].
Pharmacotherapy Interventions
Given that anxiety and depression are commonly reported in patients with asthma, particularly in severe and difficult to control disease [49], traditional pharmacologic treatment of anxiety and depression is often attempted. Both depression and anxiety in patients with asthma has been associated with poor asthma-related QOL, but depressive disorders were more commonly associated with poorer levels of asthma control [50]. The use of antidepressant medications, especially selective serotonin reuptake inhibitors (SSRIs), in this patient population has had varying success reported. One randomized placebo-controlled trial evaluated the use of citalopram in 90 adults with asthma and major depressive disorder. Not surprisingly, there was a positive effect on the primary outcome measuring depression using the Hamilton Rating Scale for Depression. Secondary outcome analysis also showed a decrease in oral corticosteroid use in the group treated with citalopram; however, no difference in asthma symptoms between groups was observed [51]. A similar but smaller RCT evaluated the use of escitalopram in major depression and severe asthma. The escitalopram group failed to show a statistical difference in depressive symptoms, asthma control, or oral prednisone use when compared with placebo [52].
The Future for Stress Management as a Fundamental Component of Asthma Care
Historically, avoidance of known triggers and use of pharmacologic maintenance and treatment modalities has been the cornerstone of asthma care. The recognition of excess psychological stress as a recognized trigger and treatment target is continuing to evolve in our therapeutic armamentarium. Our understanding of the effects of stress management in asthma patients provides clinical support for the neuroendocrine immune link between the bronchial inflammatory response characteristic in asthma and that of the human stress response. Understanding the relationships of psychological stress in asthma physiology, clinical morbidity, and therapeutic options is imperative, as the changing health care environment increasingly demands preventive, practical, cost-effective, evidence-based medicine. Some psychological stressors will no doubt be more difficult to address than others, but implementation of nonpharmacologic stress management paradigms should help improve effective asthma management across all patient demographics and should hopefully lead to decreased population health care costs, fewer days of work lost, and improved quality of life. Despite a clear molecular link between asthma, inflammation and stress and a clinical trend toward benefit, the heterogeneity of studies and poor quality evidence for each stress reduction modality make it difficult to draw any firm conclusions on the comparative efficacy of specific psychological interventions in asthma management programs. Mindfulness-based stress reduction has the highest quality evidence and shows the most promise thus far. Further research employing methodically sound RCTs that use standardized physiologic and nonphysiologic outcome measures is needed to elucidate the role for stress reduction interventions in routine clinical practice.
Corresponding author: Gailen D. Marshall Jr, MD, PhD, Div. of Clinical Immunology and Allergy, Dept. of Medicine, The University of Mississippi Medical Ctr., 2500 N. State St. N416 Jackson, MS 39216, gmarshall@umc.edu.
Financial disclosures: None.
Author contributions: conception and design, CRP, AMW, GDM; drafting of article, CRP, AMW, GDM; critical revision of the article, CRP, AMW, GDM; administrative or technical support, GDM.