Psychological Distress and Cardiovascular Disease





From the California State University, Long Beach, School of Nursing, Long Beach, CA (Dr. McGuire, Ms. Ahearn), and the University of California, Los Angeles, School of Nursing, Los Angeles, CA (Dr. Doering).
Abstract
- Objective: To review the current literature regarding psychological distress in patients with cardiovascular disease (CVD).
- Methods: Relevant and current (2005–2015) studies were retrieved by a series of searches conducted in the PubMed and PsychINFO databases using Boolean terms/phrases along with manual extraction from the reference lists of pertinent studies. Narrative and tabular summaries of the findings are reported.
- Results: There is a vast literature on psychological distress and CVD. Depression is the most common disorder studied followed by anxiety and post-traumatic stress disorder. Physiologic mechanisms linking psychological distress to CVD are well theorized. Screening for psychological distress in CVD is recommended. Referral and treatment issues need further exploration. Pharmacologic treatment of psychological distress in CVD remains equivocal; however, promising data exists for other therapies such as cognitive behavioral therapy and social support strategies.
- Conclusion: Psychological distress has a significant negative impact on patients with CVD and is underrecognized by health care providers. Primary care providers and cardiovascular specialty providers are called upon to improve their recognition of psychological distress in their patients and assure referrals are made to collaborative care teams for proper diagnosis and treatment.
The association between the heart and the mind has been proposed by scientists since the 17th century. However, it was not until the 1970s that the relationship between cardiovascular disease (CVD) and psychological states came into scientific focus. The study of heart-psyche interactions began with investigations of cardiovascular risk and “type A” personality behaviors (aggressiveness, impatience, a sense of time-urgency, intense achievement drive, seeking recognition) [1,2]. Hundreds of studies generated over the last 10 years have yielded an extensive body of literature regarding this complex interaction.
CVD continues to be the leading cause of death globally. Worldwide and in the United States, CVD accounts for 30% of deaths and more than 2000 deaths per day, respectively [3,4]. Psychological distress (specifically depression) has been reported by the World Health Organization (WHO) as the leading cause of disability in the world [4]. Taken together, CVD and depression constitute an immense health burden and result in poor health status, increased care giver burden [5], increased readmission rates to hospitals, increased utilization of primary care services, poor health compliance [6], decreased health related quality of life [7], and a greater than 2 times increase in mortality [8,9].
Despite its devastating consequences, comorbid CVD and psychological distress remains poorly recognized and treated. In this paper, we present a review of the evidence related to key aspects of psychological distress and CVD (for the purposes of this paper, defined as ischemic heart disease and stroke), and provide information to help improve identification among health care providers. Relevant and current (2005-2015) studies for this review were retrieved by a series of searches conducted in the PubMed and PsychINFO databases using Boolean terms/phrases, along with manual extraction from the reference lists of pertinent studies. Due to the breadth and extent of the literature, a comprehensive review of the literature is beyond the scope of this article. However, the reader will be directed to current systematic reviews, meta-analyses, and recent select research studies sourced for this summary and presented in tabular form.
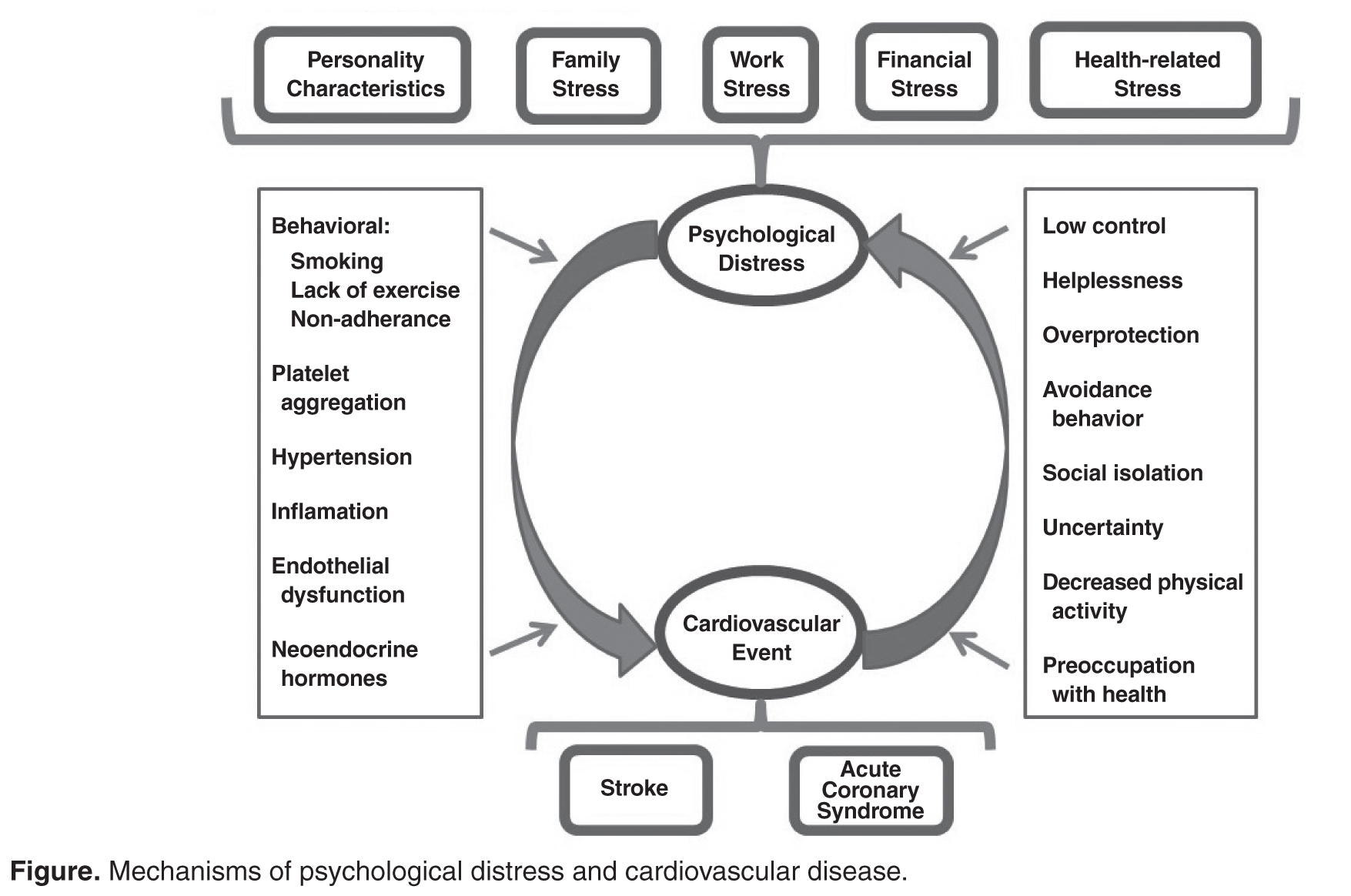
Mechanisms of Psychological Distress
Psychological Distress Disorders Related to CVD
Depression, anxiety, and post-traumatic stress disorder (PTSD) are the 3 most common psychological distress disorders related to CVD [20]. Cardiac disease and depression has been most commonly studied. In stroke, the science is not as well evolved due to greater heterogeneity of study samples and outcome measures.
Depression
Dysphoria (feeling blue), anhedonia (inability to experience joy in otherwise enjoyable activities), insomnia or hypersomnia, fatigue or loss of energy, increased guilt or worthlessness, decreased concentration, appetite change with significant weight loss or gain, psychomotor retardation or agitation, and suicidal ideation are the symptoms of depression [21]. These symptoms exist on a continuum, ranging from mild symptoms with short duration and limited functional impairment to major depression. Importantly, among otherwise healthy individuals, even minor depressive symptoms have been significantly associated with increased incidence of coronary disease [22].
Screening Issues
In recognition of the high prevalence of depression in patients with CHD, an American Heart Association (AHA) science advisory in 2008 recommended routine screening for depression in patients with CHD, with follow-up evaluation for diagnosis and treatment of depression by qualified professionals for positive cases [26]. In 2014, an AHA scientific statement recommended elevating depression to the level of a risk factor in ACS patients [27]. The recommendation for screening was initially met with some concern as being premature [28], when past supporters spoke out against the routine screening of depression in cardiac patients [29]. The dissenting authors claimed that there was a lack of scientific evidence supporting the efficacy of treatment for depression in cardiac patients, and that potential negative effects of routine screening and follow-up treatment were unknown. They argued the following: limited data from randomized controlled trials and/or evidenced-based reviews exist demonstrating improved outcomes in cardiac patients based on screening and referral [30]; antidepressants are not yet recognized to be effective in cardiac populations and there is a lack of evidence related to potential harms [28]; concerns exist about the potential for mass screening to increase health care resource use at the expense of other health care needs [29]; and routine screening may cause unnecessary negative social stigma related to false-positive findings [31].
Although clinical trials of depression treatment in cardiac patients have not demonstrated an increase in survival, treatment has been shown to be effective in reducing depression symptoms, improving patient satisfaction with depression care and improving health related quality of life [32–34]. Further, recent studies described the AHA recommendation as well accepted by cardiac unit staff, not heavily resource intensive, feasible, and accurate [35,36]. Bigger and Glassman [37] published a recent analytical review of the AHA advisory and concluded that the advisory is supported by the literature. A salient point regarding the depression screening debate is that screening without proper follow-up for further diagnosis and potential treatment may be harmful [28,29,31]. Despite concerns of the potential negative impact of depression screening in cardiac patients raised in the literature, the preponderance of the literature indicates that its benefits are likely to outweigh its risks [32,34,36,38–40].
Outcomes of Depression Treatment
Answers to questions about improvement in cardiovascular and all-cause mortality outcomes with depression treatment remain elusive in the literature. However, data show an improvement in depressive symptoms and quality of life for depressed patients receiving some types of treatment [33,41–45]. The Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) study was a landmark study of MI patients with a 6-month treatment intervention of cognitive behavioral therapy (CBT) plus pharmacologic intervention if indicated for depression [33]. Patients were followed for an average of 29 months post-MI. A significant improvement was seen in depressive symptoms and social isolation in the treatment group; however, there was no improvement in event-free survival [33]. When outcome measures are restricted to mortality alone, subsequent trials of antidepressant medications for treatment of depression in cardiac patients have shown them to be ineffective [46]. However, CBT and other supportive stress management strategies are effective in decreasing depressive symptoms and improving the quality of life in patients suffering with depression and CVD [46].
Promising results are emerging in the literature as researchers refocus their analysis on subgroups of depressed cardiac patients. In one large study of 442 depressed and 325 non-depressed patients, the number of depressive symptoms after an MI irrespective of the pre-MI depression status was associated with worse cardiac outcomes [47]. For every 1 additional depressive symptom reported 1 year post-MI, patients had a 15% increased risk for a new cardiac event in the next 2.5 years [47]. Another study demonstrated an improvement in depressive symptoms by 75.3% in in post-cardiac surgery patients with low ejection fraction (< 40%) after 8 weeks of nurse-guided CBT and worsening in depressive symptoms by 26.8% in usual care patients. More moderate findings were seen in the those with higher ejection fraction receiving the same CBT intervention for depression [45]. A treatment-resistant depression subgroup analyzed in a recent secondary analysis of the ENRICHD trial showed a twofold increase in mortality when compared to those in the non–treatment-resistant depression group [48]. Since treatment does not work for all patients with depression, including depressed post-MI patients, further evaluation with a focus on those who respond to treatment is needed.
Depression in Stroke
Issues related to treatment of stroke patients parallel those of depressed patients with cardiac disease, as the effect on mortality and survival is unknown. Depression has been reported to go untreated in up to 67.9% of depressed post-stroke patients [54]. In addition, mismatches between antidepressant prescription and those with depression suggested that some patients without depression were being treated for depression while some patients with depression were not being treated [54].
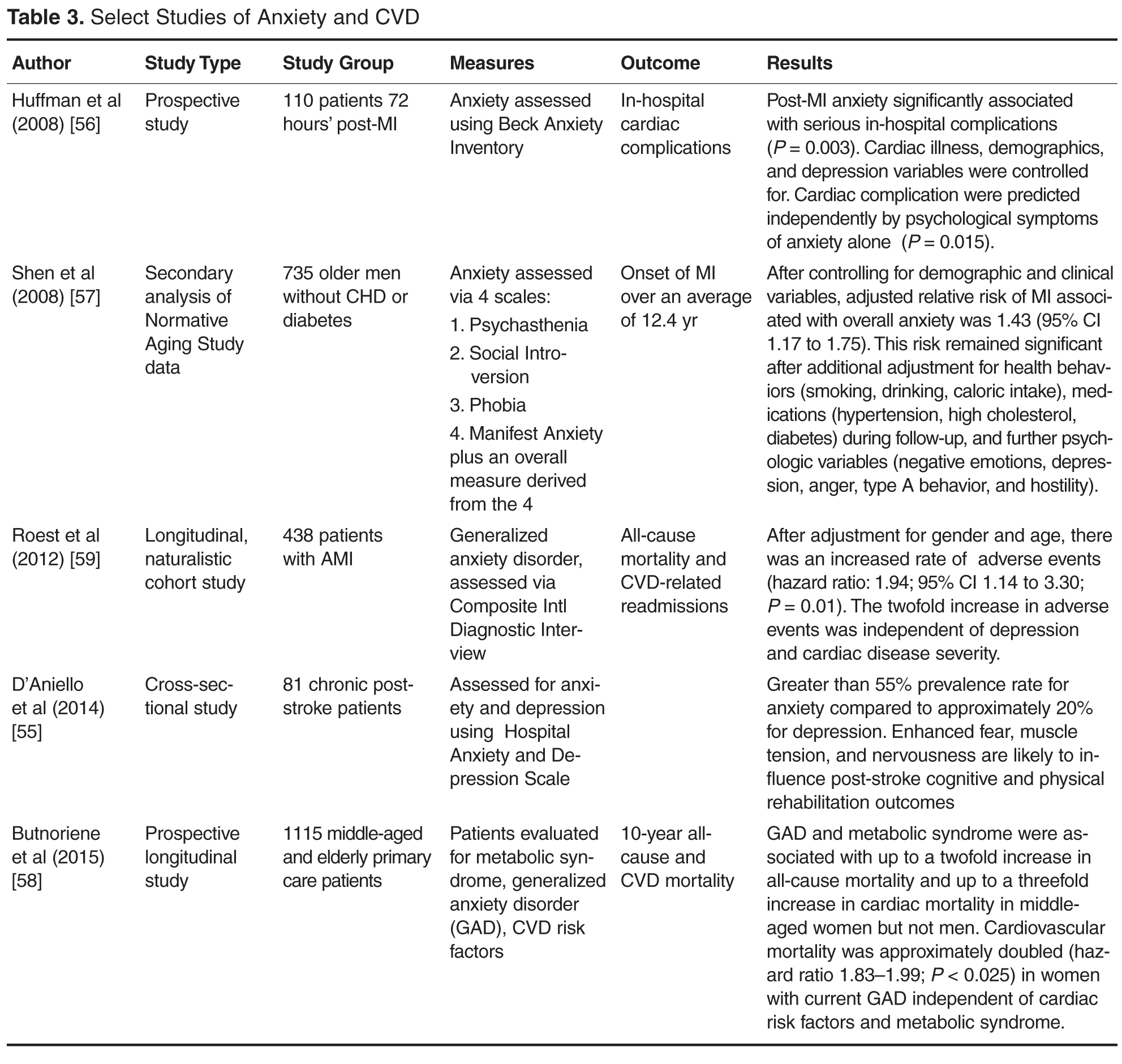
Anxiety
Anxiety disorders create behavioral disturbances of fear and avoidance related to an individual’s propensity to overestimate dangers [21]. Though a number of anxiety disorders are described in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), anxiety as a general constellation of symptoms (afraid, inability to relax, worry about everyday problems, feelings of panic) is described in most of the literature related to CVD [55–57]. To a lesser extent, generalized anxiety disorder (GAD), defined as anxiety symptoms on more days than not and lasting more than 6 months [58,59] has also been studied. Because anxiety can be a component of depression, the 2 are often discussed together. Taken together, in the context of CHD, individuals with both anxiety and depression are at significantly greater risk for death (odds ratio 2.35, 95% confidence interval 1.23-4.47, P =0.01), compared with those without symptoms [60].
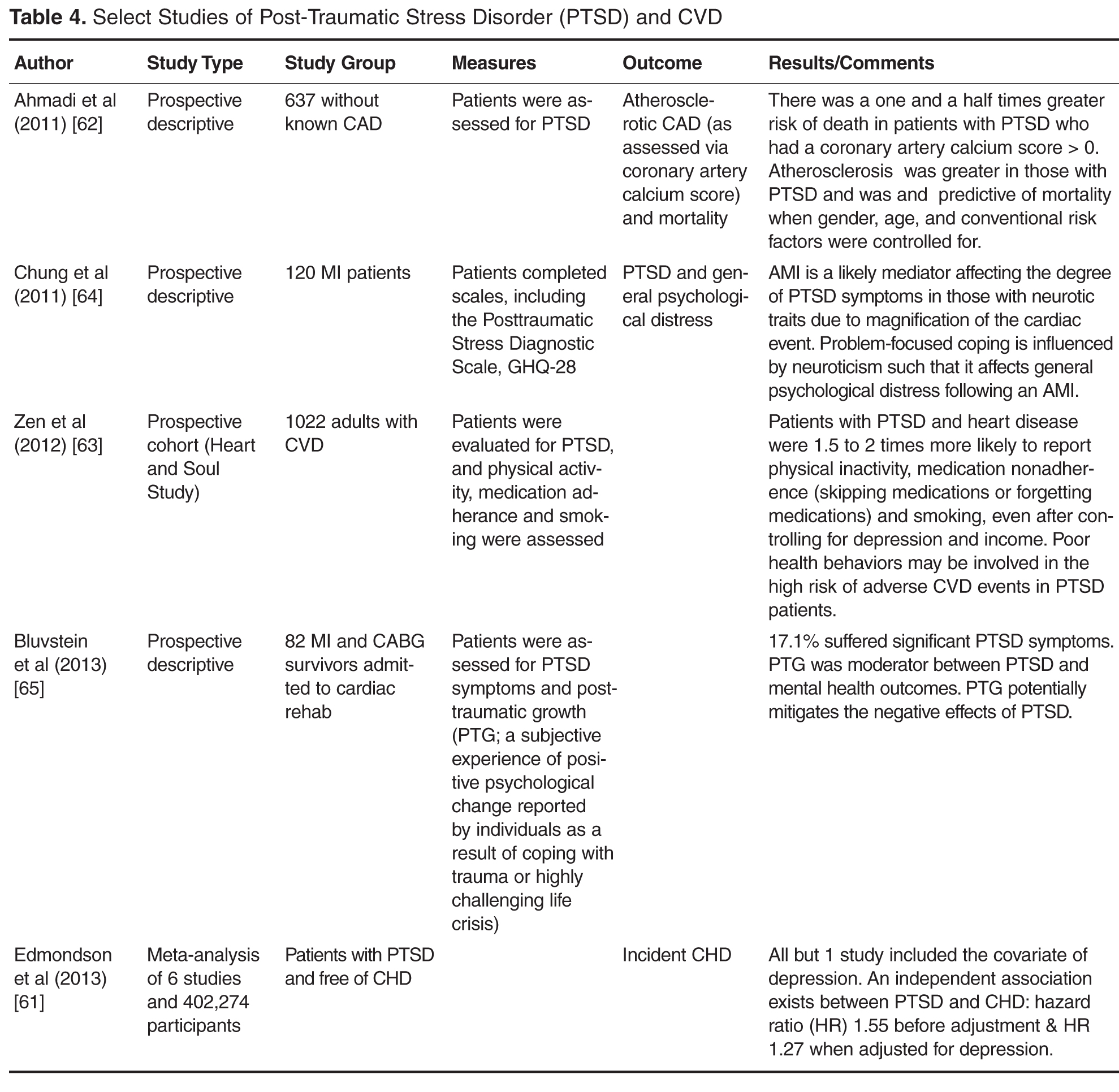
Post-Traumatic Stress Disorder
PTSD presents with a heterogeneous cluster of symptoms that are generally described as avoidance, re-experiencing, arousal, and negative cognitions and mood [21]. Previously classified as a anxiety disorder in DSM-IV, PTSD is in a new category of trauma and stress or related disorders in the revised DSM-V [21]. In addition, the temporal component of the symptoms has been changed to a disturbance lasting more than 1 month, without reference to acuity or chronicity.
Implications for Clinical Practice
Despite the extensive body of literature regarding the negative association of psychological distress to health outcomes in CVD patients, there remains a significant practice gap related to screening, referral, and treatment of psychological distress in CVD patients [30,36,66]. Busy clinical practices focused on physical symptoms (which may not be recognized as mental health–related), along with a health system that has historically regarded mental health issues as the sole domain of mental health professionals creates barriers that need to be overcome. Many health care providers are not proactive in screening patients for psychological distress [11]. Additionally, psychological distress is often perceived as a metaphysical, inexact phenomenon, and is not regarded with the same import as physiological indices, such blood pressure and lipid levels [13]. Another significant barrier may be that the importance of psychological distress, especially depression, has been minimized by some investigators and clinicians because of the lack of data that show improvement with treatment of “hard” outcomes, such as mortality. Lastly, no studies have conclusively demonstrated that treating depression in the general population would lower subsequent cardiovascular clinical events, adding to the minimization of the importance of screening, referral, and treatment of psychological distress among clinicians.
The challenges associated with psychological distress and CVD are centered on the perceived role of the health care provider and role of the patient [11,67]. To date, identification of patients with psychological distress in CVD populations has not been considered a part of routine practice, and only a small percent of those identified with psychological distress are treated. In one study, 17.6% of 1181 patients had moderate to severe depression and of those, only 24.5% were recognized as depressed by their health care providers [68]. In a smaller study of 35 patients with depression after an acute MI, only 10% received treatment with antidepressants [66]. Similarly poor treatment rates were seen in a recent study of antidepressant use after stroke and transient ischemic attack (TIA), with 67.9% of stroke patients and 70.0% of TIA patients with persistent depression going untreated [54].
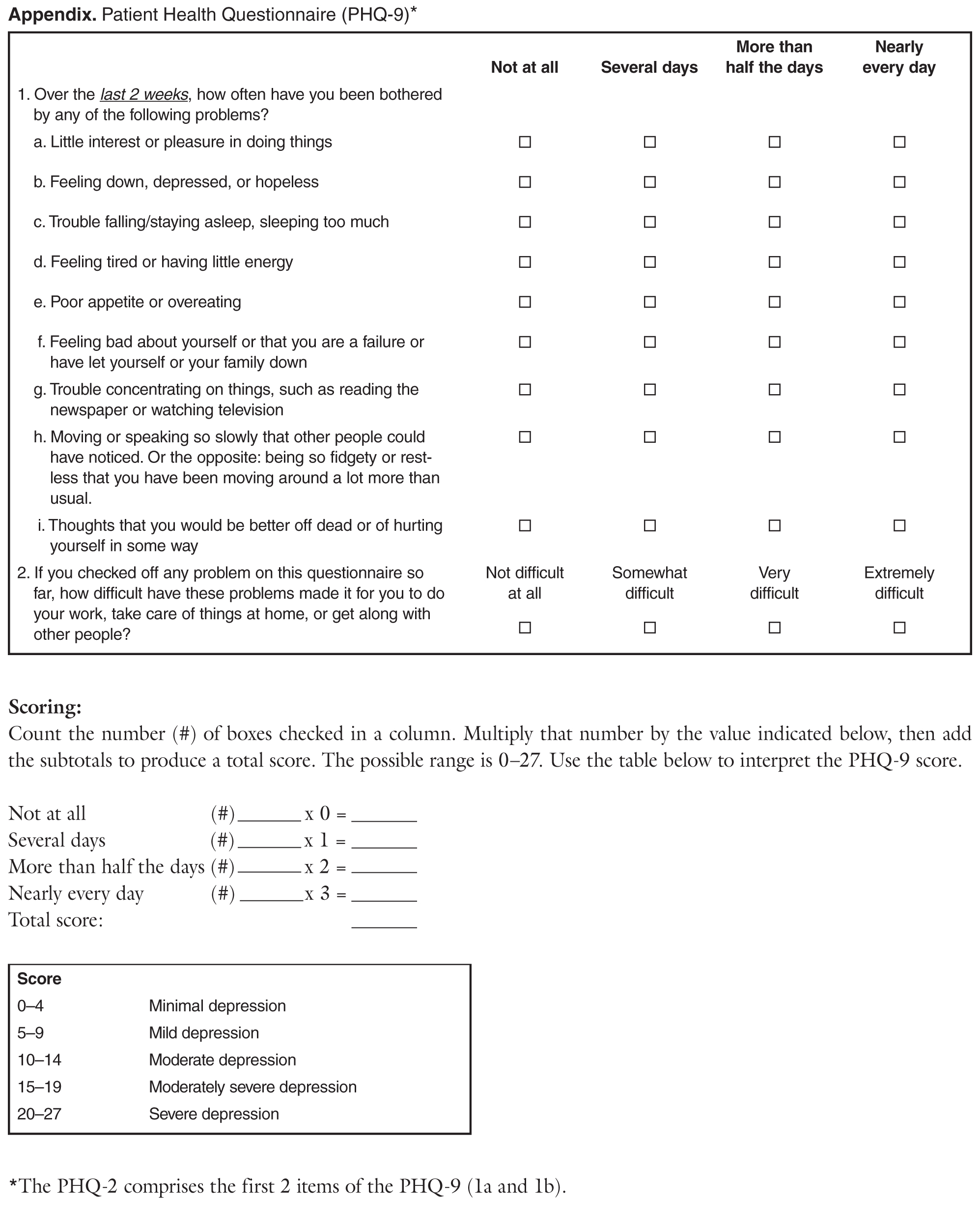
Stress, depression, anxiety, and PTSD are often not self-contained or experienced in isolation. Rather, some or all of these conditions may present as an interconnected phenomenon [69,70]. There are several reasons for this. First, symptom identification relies on self-report and/or observation of the symptoms, which may confound validity and reliability of diagnosis [70]. Second, the conditions share some symptoms, which may complicate diagnosis of a primary condition. In addition, the overlap of somatic, cognitive, and affective symptoms [71] may deter health care providers from using screening tools that have physical symptoms as part of the screening process. In a recent study of depressed cardiac patients, investigators clustered symptoms and demonstrated that cognitive affective symptoms of depression predict depression in patients with heart disease [72]. Certain events, such as stroke, may make screening especially difficult due to the presence of neurological changes that may complicate the screening process [73]. These issues highlight the need for formalized depression screening tools such as the Patient Health Questionnaire 2-item screening tool (PHQ-2) and/or Patient Health Questionnaire nine-item screening tool (PHQ-9) (Appendix), as recommended by the AHA. The PHQs have been validated in stroke patients and cardiac patients and have been found to be accurate, easy to use, and feasible [35,36,73].
Patients look to their providers for information and security during vulnerable times in their life. In a 2014 study regarding the perceptions of psychosocial consequences and access to support after MI, patients reported a high sense of security regarding being able to contact their providers [74]. Providers in both the primary and acute care settings should use these opportunities to assess for psychological distress. Many inpatient health care providers assume that it is the primary care providers’ responsibility to screen for depression [75]; however, screening should be done in all practice settings caring for patients with CVD. Clinical practice environments should develop policies and procedures to define who, when, and how screening for psychological distress is accomplished using currently available brief screening tools.
A plan for insuring that proper referrals are made following screening to ensure accurate diagnosis, effective treatment, and follow-up should be in place. To date, there is ample evidence that patients benefit from screening in the context of an interdisciplinary treatment approach [34]. Collaborative care, utilizing a team of health professionals (physician, case manager trained in working with patients with psychological distress, and mental health specialist) working with the patient, is an ideal model to improve outcomes [44]. A Cochrane review of 79 RCTs with over 24,000 participants compared utilization of a collaborative team with routine care and found decreased depression and anxiety symptoms in patients receiving team care for up 2 years, along with improved medication adherence, improved quality of life, and improved patient satisfaction with care [39].
Conclusion
Psychological distress remains underrecognized in CVD patients. Brief screening tools such as the PHQ-2 and PHQ-9 are available, easy to use, and reliable for use by clinicians to improve case finding. Primary care providers and cardiovascular specialty providers are called upon to improve the recognition of psychological distress in their patients and assure referrals are made to collaborative care teams for proper diagnosis and treatment of mental health issues. Longitudinal studies focused on the impact of primary/secondary/tertiary psychological distress prevention strategies in the general population, as well as those with CVD, are needed to bring the state of the science forward and provide evidence to enhance the care of those with psychological distress and CVD.
Corresponding author: Anthony McGuire, RN, PhD, ACNP-BC, CSULB, School of Nursing, #2 1250 Bellflower Blvd., Long Beach, CA 90804, Anthony.McGuire@csulb.edu.
Financial disclosures: None
Author contributions: conception and design, AWM, EA, LVD; drafting of article, AWM, EA, LVD; critical revision of the article, AWM, EA, LVD; collection and assembly of data, AWM, EA, LVD.