Assessment of False-Positive Fentanyl Results on Urine Drug Screens in Veterans





Background: False-positive fentanyl results on a urine drug screen (UDS) can significantly impact treatment, health care costs, and patient quality of life. Limited research exists on the impact and frequency of false-positive fentanyl results using the current testing assay.
Methods: This retrospective, multicenter analysis included patients with positive fentanyl UDS results at 3 US Department of Veterans Affairs MidSouth Healthcare Network facilities in Tennessee from August 1, 2023, to August 1, 2024. The primary outcome was the rate of false-positive results for fentanyl on confirmation testing. Facilities 1 and 2 used a 1 ng/mL cutoff, while facility 3 used a 2 ng/mL cutoff. Secondary outcomes included rate of confirmation testing, prescribed medications for patients with false-positive results, and the rate of follow-up on confirmation results.
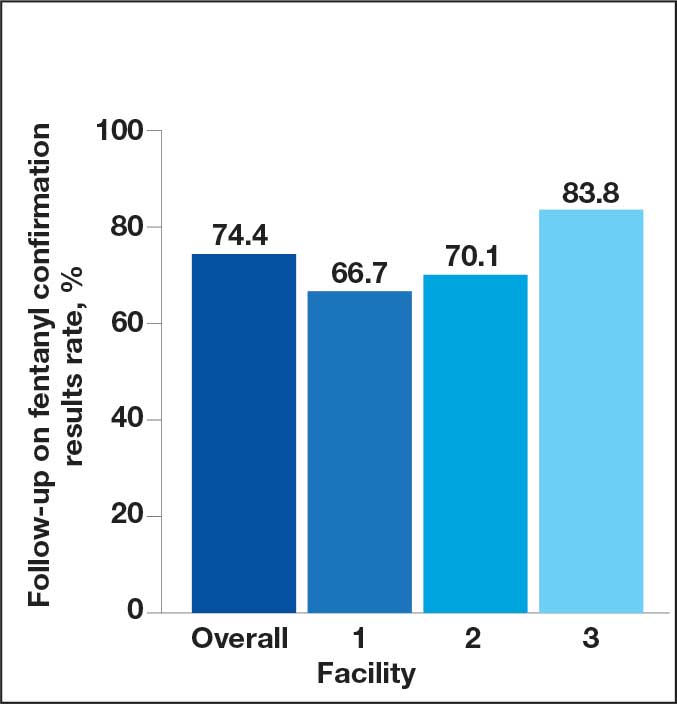
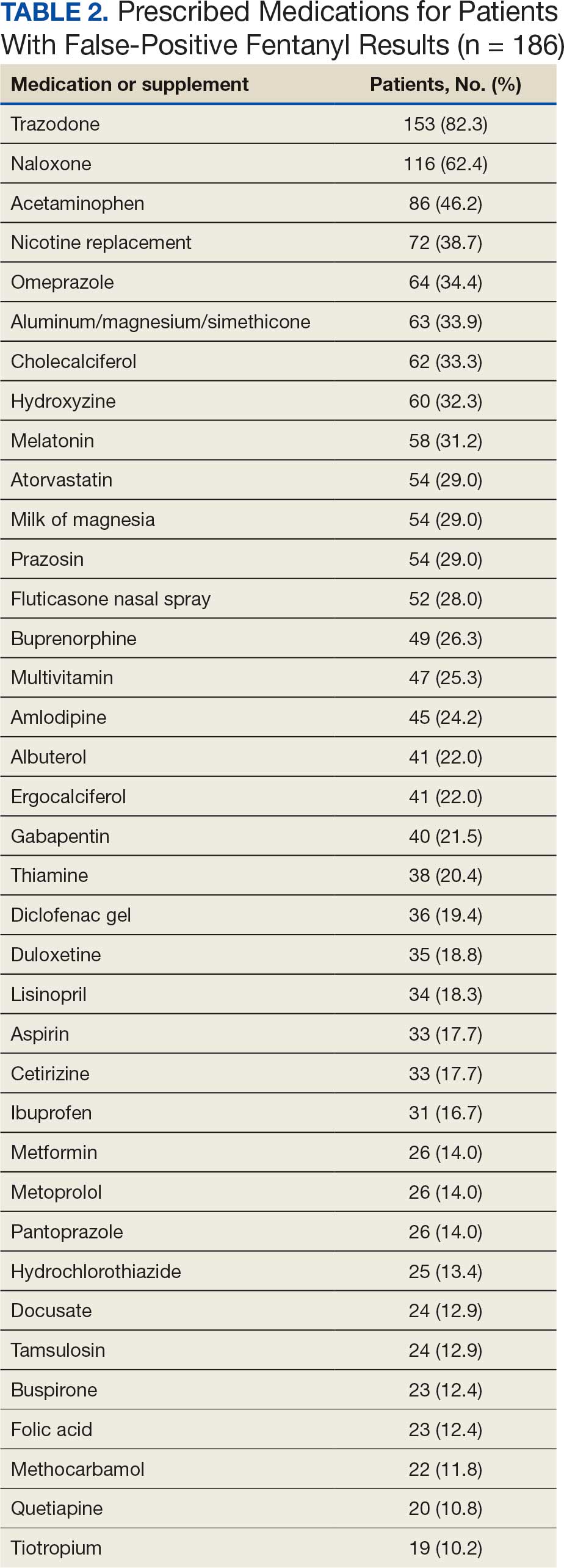
Results: A total of 1228 UDS samples were included. Of these, 578 (47.1%) were sent for confirmation: 87 (15.1%) at facility 1, 277 (47.9%) at facility 2, and 214 (37.0%) at facility 3. A total of 546 (94.5%) had confirmation results. The false-positive rate based on confirmation testing was 49.9% at facilities 1 and 2, and 4.7% at facility 3. Clinicians followed up on 74.4% of confirmation results (66.7% at facility 1, 70.1% at facility 2, and 83.8% at facility 3). Trazodone was prescribed to 153 patients with false-positive results (82.3%).
Conclusions: There was a high rate of false-positive fentanyl results, suggesting the need for automatic confirmation testing for verification. These findings resulted in facility 1 switching to automatic confirmation testing. The high rate of trazodone use among patients with false-positive results adds to data implicating trazodone in false-positive fentanyl UDS results.
A urine drug screen (UDS) is commonly performed to evaluate illicit and prescribed drug use in patients to guide treatment decisions and ensure patient safety. Common uses include evaluating medication adherence, identifying ingested substances in cases of intoxication or overdose, ruling out substance-induced disorders, and screening for illicit drug use. There is a potential for false-positive or false-negative results due to the qualitative and nonspecific nature of UDSs.1 These results can be verified with confirmatory testing using gas chromatography/mass spectrometry or liquid chromatography/ tandem mass spectrometry by identifying specific molecular structures and quantifying the amount of drug or substance present in the sample.1
An April 2023 memorandum instructed all US Department of Veterans Affairs (VA) medical centers and community-based outpatient clinics (CBOC) to have fentanyl urine testing readily available.2 Some facilities added fentanyl to a standard UDS, while others created a separate quick order. The memorandum led to increased fentanyl testing. As a result, unexpected positive fentanyl UDS results are more common. Some facilities have an automatic fentanyl confirmation test that is ordered after a positive fentanyl UDS. However, a positive result for fentanyl on a UDS does not automatically result in confirmation testing at all VA facilities. Without automatic confirmation testing, a clinician must decide to order a fentanyl confirmation test following the positive result. Therefore, the true rate of false-positive results for fentanyl is unknown because confirmation testing is not ordered for every positive UDS.
False-positive results can have unintended consequences, including discontinuation of prescribed medications, patient stigma, and inappropriate recommendations for substance use treatment. False-positive results may contribute to unnecessary health care costs and adversely affect patients’ lives. Previous research has reported false-positive fentanyl UDS results for patients taking risperidone, ziprasidone, and labetalol.3-5 Studies have found that loperamide and high-concentration methamphetamine samples could cause false-positive fentanyl UDS results.6,7 Wang et al evaluated the performance of the SEFRIA fentanyl immunoassay using the 1 ng/mL cutoff cleared by the US Food and Drug Administration (FDA). The study of 410 patients found a 38% false-positive rate; concomitant use of trazodone, labetalol, and haloperidol accounted for 230 (56%) of the false-positive results.8 Limited data evaluating false-positive results for the current SEFRIA fentanyl testing assay suggest the need for additional research. This study aims to add to data on false-positive results for fentanyl on UDS samples and potential causes.
Methods
A retrospective, multicenter observational cohort study was conducted that included patients at 3 VA MidSouth Healthcare Network VA medical centers located in Tennessee with their associated CBOCs from August 1, 2023, to August 1, 2024 who had positive fentanyl UDS results. The primary outcome was the rate of false-positive fentanyl UDS results when confirmation testing was performed. Secondary outcomes included the rate of confirmation testing, prescribed medications used by patients with false-positive UDS results, and the rate of follow-up in the electronic health record (EHR) on results of confirmation testing. Confirmations were primarily obtained for positive results and not all UDSs. Therefore, it was not possible in this retrospective study to obtain the true measure of false-negative or true-negative results.
A structured query language query was performed to identify patients with a UDS positive for fentanyl from August 1, 2023, to August 1, 2024. Patients were enrolled if they were aged ≥ 18 years with a UDS positive for fentanyl. Patients were excluded from the primary outcome analysis if results for the confirmatory testing were unquantifiable or could not be found.
Study Intervention
This was a descriptive study with no comparator group. The rate of confirmed false-positive results for fentanyl, rate of confirmation testing for patients with positive fentanyl UDS results, rate of follow-up on confirmation results, and prescribed medications in patients with false-positive fentanyl results were evaluated. For true-positive results, follow-up was defined as documentation in the EHR reporting fentanyl use or illicit substance use likely to be laced with fentanyl at the time of the UDS or documentation of the confirmation result. For false-positive results, follow-up was defined as documentation in the EHR of the confirmation result.
Statistical Analysis
Descriptive statistics including means and percentages were used to analyze demographic data. Continuous variables and parametric data are presented as mean (SD) and nominal data as percentages. All statistical analyses were completed using Excel. The SEFRIA fentanyl immunoassay was used at each study site. Facilities 1 and 2 were combined for the primary outcome analysis because they used the same fentanyl immunoassay cutoff level of 1 ng/mL. Facility 3 used a cutoff level of 2 ng/mL and was analyzed separately.
Results
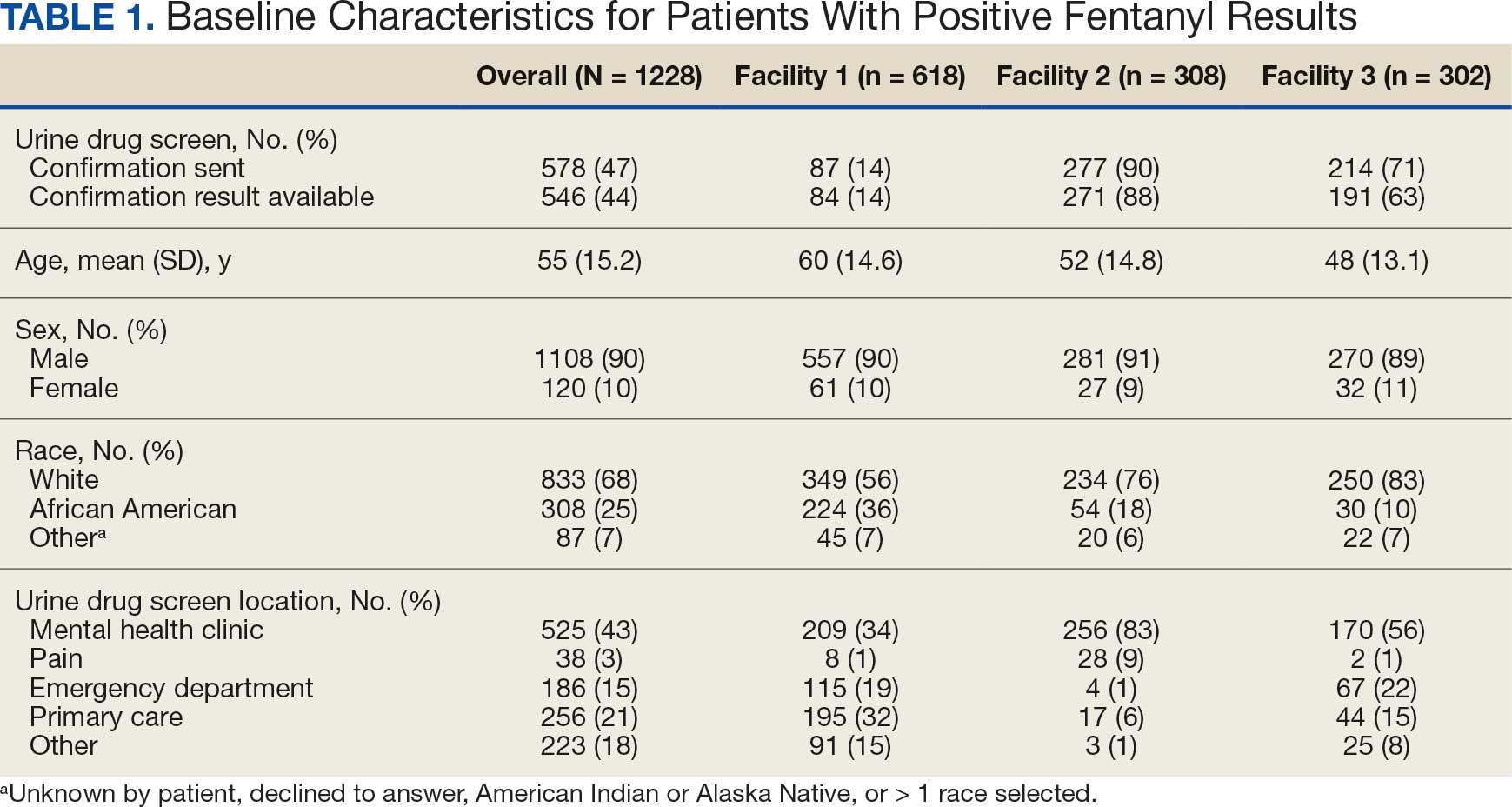
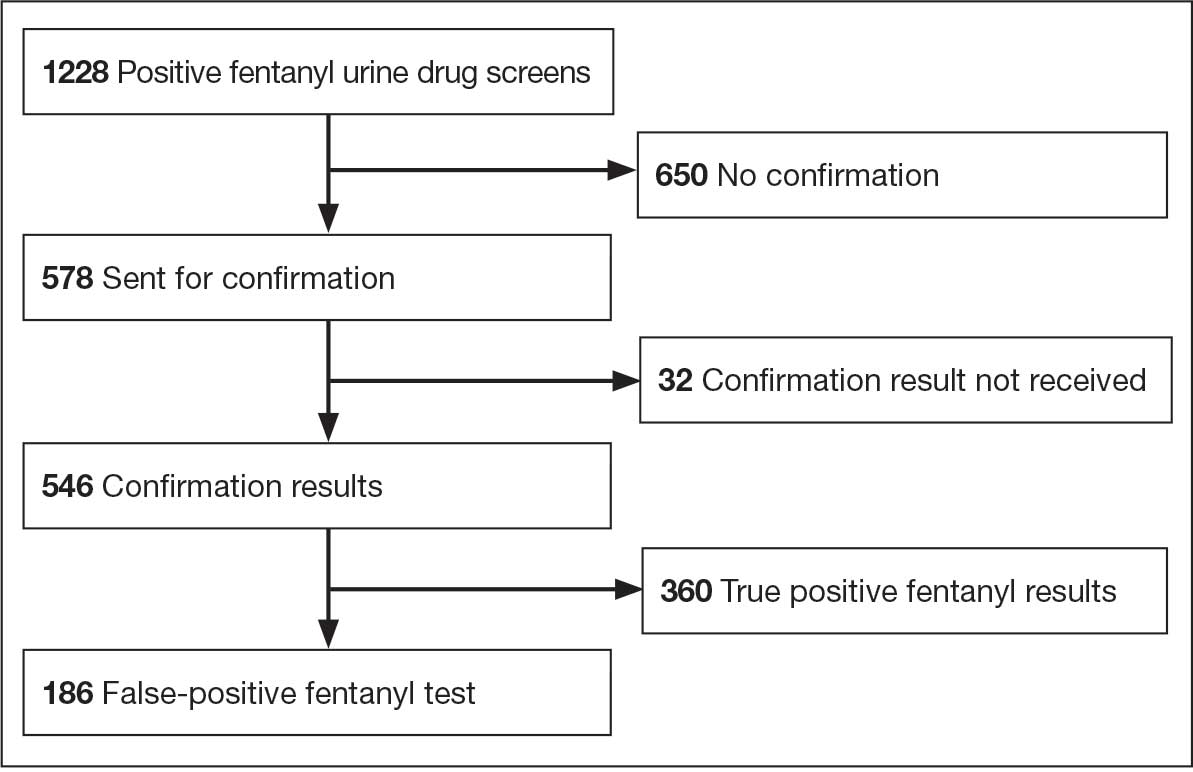
A total of 1228 UDS tests were positive for fentanyl, including 618 at facility 1, 308 at facility 2, and 302 at facility 3 (Figure 1). Patients were predominantly male and White, with a mean age of 55 years, though age and race varied by location (Table 1). Patients may have had ≥ 1 UDS. Of 1228 UDSs recorded in the EHR, 578 were sent for confirmation testing and 546 had confirmation results available in the EHR (84 at facility 1, 271 at facility 2, and 191 at facility 3). Of 546 confirmation tests, 186 were negative for fentanyl, indicating a false-positive rate of 34.1%. Most confirmation tests (43%) were requested for patients seen in a mental health clinic.
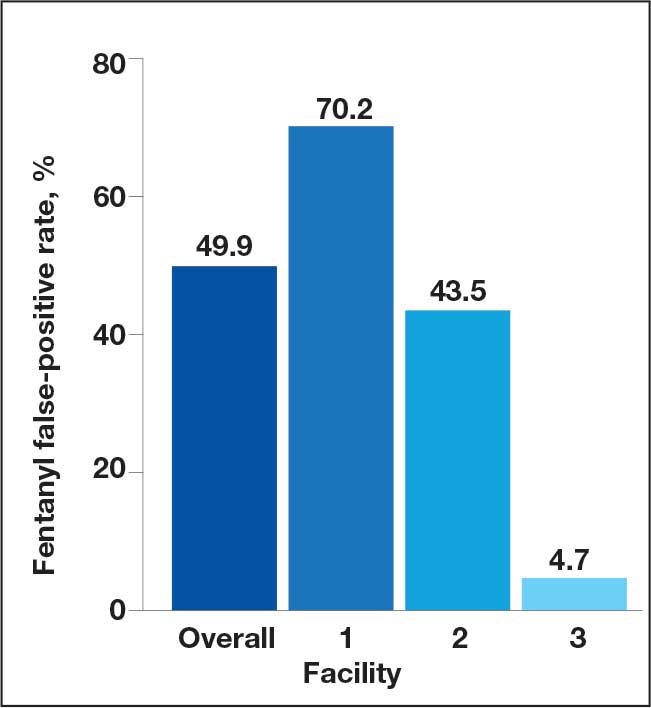
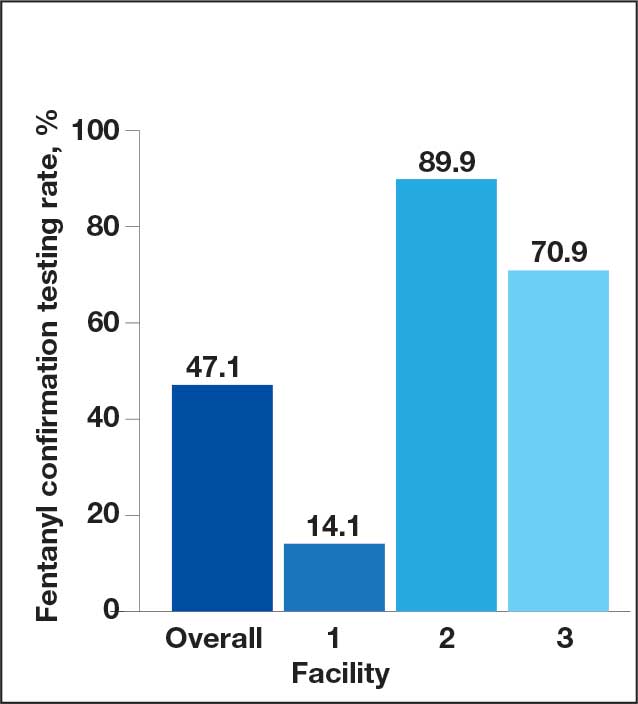
The combined false-positive rate was 49.9% for 355 UDS confirmation results at facilities 1 and 2 (70.2% and 43.5%, respectively) and 4.7% for 191 UDS confirmation results at facility 3, which used the higher 2 ng/mL cutoff level (Figure 2). Confirmation testing was ordered for 578 tests (47.1%). There were 87 confirmation tests (14.1%) at facility 1, 277 tests (89.9%) at facility 2, and 214 (70.9%) at facility 3 (Figure 3). Follow-up after confirmation tests was completed for 406 patients (74.4%): 56 follow-ups (66.7%) at facility 1, 190 follow-ups (70.1%) at facility 2, and 160 follow-ups (83.8%) at facility 3 (Figure 4). Trazodone was the most commonly prescribed medication for patients with false-positive fentanyl UDS results. Trazodone was prescribed to 153 patients (82,3%), followed by 116 patients (62.4%) prescribed naloxone, 86 patients (46.2%) prescribed or with reported use of acetaminophen, 72 patients (38.7%) prescribed nicotine replacement products, and 64 patients (34.4%) prescribed omeprazole (Table 2).
Confirmed Fentanyl False-Positive Rate
Confirmation Testing
Fentanyl Confirmation Results
Discussion
There are several factors to note when interpreting the study results. First, facilities 1 and 2 used the FDA-cleared 1 ng/mL cutoff for positive results on the SEFRIA fentanyl immunoassay, whereas facility 3 used a cutoff level of 2 ng/mL. Second, during the study period, facilities 1 and 3 included fentanyl as part of their standard UDS; facility 2 required a separate fentanyl UDS order. Third, facility 2 had automatic confirmation testing for positive results on individually ordered fentanyl UDS tests. Finally, confirmation tests were primarily obtained for positive fentanyl results and not all UDSs, which limited the analyses that could be performed.
This study found a high rate of false-positive fentanyl UDS results at facilities 1 and 2 and a very low rate at facility 3, likely due to the higher cutoff level. Facility 3 used the higher cutoff level due to previously observed high rates of false-positive results. While a higher cutoff level can decrease the rate of false-positive results, it also may increase the rate of false-negative results.
Studies have found false-positive rates ranging from 3% to 45% with the SEFRIA immunoassay FDA-cleared 1 ng/mL cutoff. Increasing the cutoff to 1.3 ng/mL decreased the false-positive rate from 38% to 7.5% in a study by Wang et al.8-11 Manar et al evaluated fentanyl assays in 42 samples using a 2 ng/mL cutoff for the SEFRIA assay and reported a false-positive rate of 0 and a false-negative rate of 22.5%.12 Given the high rate of false-positive rates demonstrated in studies using the current FDA-recommended 1 ng/mL cutoff, additional studies evaluating different cutoff levels may be beneficial to determine the best cutoff level to reduce false-positive results without significantly increasing false-negative rates. While data on the impact of using a higher cutoff level are limited, the results of our study have led to discussions at VA MidSouth Healthcare Network facilities regarding use of different cutoff levels.
There was a low rate of confirmation testing at facility 1 compared with facilities 2 and 3. Only facility 2 had automatic confirmation testing during the study period. Pharmacists at facility 3 reviewed UDS results without needing a consultation and, during the study period, could order fentanyl UDS confirmations. Another factor that may have contributed to the disparity in confirmation testing between facilities is the location of the UDS order. Most UDS samples at facilities 2 and 3 were ordered for patients seen in mental health clinics, whereas many facility 1 orders were placed in primary care or the emergency department (ED).
Given these results, education may be indicated regarding the risk of false-positive results and the importance of confirmation testing in primary care and the ED. Facility 1 and 3 did not have automatic fentanyl confirmation testing during the study; however, facility 3 implemented automatic confirmation shortly after the study period and facility 1 implemented automatic confirmation testing for a positive fentanyl UDS result after evaluation of the study data.
Although follow-up on confirmation UDS results was fairly high, it was highest at facility 3, which does not require a consultation for pharmacist UDS result evaluations. Given the high rate of false-positive results for fentanyl, confirmation testing for a positive UDS and follow-up on confirmation results is an important step to consider. The higher rate of follow-up at the facility where pharmacists had more autonomous involvement shows the benefits of having pharmacists provide comprehensive patient care. Implementing similar protocols across all facilities may improve follow-up, which may improve patient care and safety given the implications of false-positive results.
Trazodone was prescribed in 82.3% of all patients with false-positive fentanyl tests. Even at facility 3, with the higher fentanyl immunoassay cutoff level, trazodone was prescribed in 77.8% of patients with false-positive results. While this retrospective study does not show causation, it does align with the findings reported by Wang et al, adding to the data implicating trazodone as a potential cause for false-positive fentanyl UDS results. The high incidence of trazodone prescriptions in patients with false-positive UDS results at facility 3 strengthens this association, indicating that even when using a higher cutoff level, trazodone may be implicated.
While there was a high rate of confirmed false-positive results in this study, there was also a potential for undetected true-positive results. The SEFRIA fentanyl immunoassay is sensitive to multiple fentanyl analogues. Williams et al showed that the SEFRIA immunoassay detected 57 of 58 fentanyl analogues tested; norsufentanil was the only analogue it did not detect.13 Most of the confirmatory tests reviewed during this study did not include all fentanyl analogues, only fentanyl and norfentanyl. Given the increased prevalence of synthetic fentanyl analogues, this is an important consideration because some identified false-positive results could potentially be undetected true-positive results for a fentanyl analogue. Switching to a more comprehensive confirmation test that includes more fentanyl analogues may reduce the risk of undetected positive results and, therefore, reduce the observed rate of false-positive UDS results.
Strengths and Limitations
Patient medications were only identified if they were documented in the EHR at the time of UDS results, which could have missed over-the-counter medications or medications prescribed outside the VA; this limits identification and implication of medications as possibly contributing to false-positive results. Only samples sent for confirmation were evaluated for true- or false-positive results; therefore, the true rate of false-positive results could not be determined. UDS confirmation tests only analyzed for fentanyl and norfentanyl, which left the potential for undetected true-positive results for other fentanyl analogues. Use of EHR data for the analysis leaves the potential for documentation errors and undetected bias.
This study adds to limited data on false-positive results for fentanyl on UDS samples. It included a large sample size of patients across multiple sites. Additionally, it included results using multiple cutoff levels on the SEFRIA fentanyl immunoassay, adding to limited data in this area.
Conclusions
This retrospective study found evidence that automatic confirmation testing should be considered for positive fentanyl UDS tests due to the high rate of false-positive results. Facility 1 began automatic confirmation testing due to the findings of this study. Facilities should consider switching to a more comprehensive confirmation test that includes more fentanyl analogues to reduce the risk of undetected true-positive results. This study also adds to the data implicating trazodone in fentanyl UDS false-positive results due to high incidence of trazodone prescriptions among patients in the study with false-positive UDS results. Future considerations include investigating different cutoff levels for the SEFRIA fentanyl immunoassay to reduce false-positive results as data are currently limited.