An Opportunity to Provide High-Quality Training and Care: Use of Telesupervision and Reflection on Practices





Background: Rural populations experience more health care disparities than urban populations, including higher rates of chronic conditions and limited access to health care practitioners and facilities. Because health care professional (HCP) training programs are largely based in urban areas and often shape where early-career clinicians practice, rural communities have fewer opportunities to attract individuals to build sustainable local workforces. As the largest provider of health professions training, the US Department of Veterans Affairs (VA) is well positioned to leverage telesupervision— clinical supervision delivered via synchronous audio and video—to strengthen rural training, support high-quality care, and enhance workforce retention.
Observations: This 3-year quality improvement project analyzed 11 rural VA psychology training programs. A total of 3197 monthly questionnaires from supervisors and trainees showed that telesupervision upheld patient safety and supervision quality while increasing trainees’ comfort with telehealth care. These findings illustrate how telesupervision can create new opportunities to maintain high-quality training and care by connecting geographically dispersed health care practitioners. The evolving use of telesupervision underscores that clinical supervision is a distinct competency requiring intentional relationship building, direct observation, and structured feedback.
Conclusions: Thoughtfully implemented telesupervision can support safe, high-quality supervision while broadening access to rural training experiences and specialty expertise. For rural VA sites, telesupervision may strengthen supervisors’ professional connection, increase trainees’ engagement with veterans living in rural communities, and contribute to rural workforce sustainability and improved population health.
Rural populations experience more health care disparities than urban populations, including a greater proportion of adults aged ≥ 65 years, higher poverty, and a higher prevalence of chronic comorbidities. Reported rates vary by study methodology and over time.1 These disparities are further exacerbated by reduced access to health care practitioners (HCPs), particularly physical and mental health specialty services, and a lack of rural health care facilities.1 HCP training programs are primarily located in urban settings and may heavily influence the geographical location and population focus of newly trained HCPs’ first positions.2 As the largest provider of health professions training, the US Department of Veterans Affairs (VA) can innovate to improve the quality of education and training while supporting rural health care sustainability and health care workforce retention.3,4
One such innovation is expanding the implementation of telesupervision (ie, clinical supervision delivered via synchronous audio and video formats) for health professions trainees. During the COVID-19 pandemic, the literature documenting telesupervision substantially expanded across health care disciplines. These findings support telesupervision as a feasible alternative to traditional in-person supervision and suggest increased trainee comfort with telehealth use.5,6 The literature also provides insight into considerations for the use of telesupervision, including being more intentional in the development of the supervisory relationship,6-8 and enabling appropriate access to supervisors to support quality patient care and experiential learning.9,10
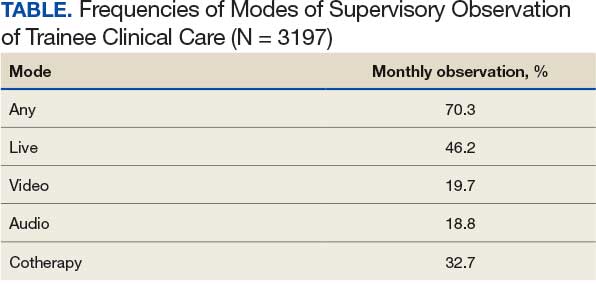
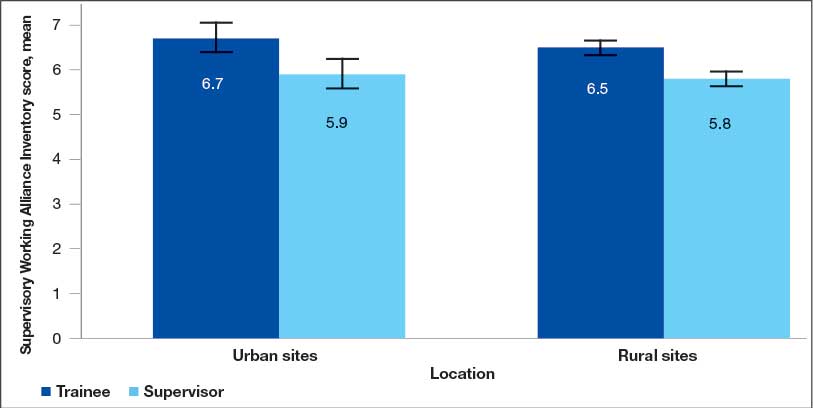
This quality improvement examination of telesupervision in 11 rural VA psychology training programs spanned 3 years and included 3197 monthly surveys completed by supervisors and trainees. It supported the use of telesupervision compared with in-person or mixed modality supervision across a wide range of outcomes in upholding patient safety and maintaining the quality of supervision while also expanding trainees’ comfort in implementing telehealth care. The Table summarizes how frequently supervisors observed trainees providing clinical care via live observation, video or tape reviews, or conducting cotherapy. The clinical sessions for most trainees (70.3%) were directly observed by supervisors at least monthly across all methods. We also reviewed differences in Supervisory Working Alliance Inventory (SWAI) scores, which quantify the strength of the working relationship between trainees and supervisors, across 458 rotations by position (trainee vs supervisor) and rurality (rural vs urban sites). Overall, alliance was high with mean scores of 5.5 to 6.7 on a 7-point scale. While trainees tended to report higher alliance (P < .001), there were no differences by rurality (P = .06) or the rurality × position interaction (P = .08), and the marginally significant effects were small, indicating that rurality tended to attenuate position effects (Figure). Additional analyses of modality (in-person, telesupervision, or mixed modalities) indicated no differences. Thus, trainee and supervisor data from this project identified safe, high-quality, and consistent supervisory practices. Finally, additional data highlighted the potential benefits of a mixed-modality supervision, including both in-person supervision and telesupervision.11,12
The expanded use of telesupervision provides several new opportunities for rural health care clinical supervisors, trainees, and veterans. Clinical supervisors who would otherwise operate as the sole HCP within their discipline or specialty at a remote clinic can increase their professional connection to a main facility and/or larger professional organization by serving as a clinical supervisor within a training program via telesupervision. This creates a greater connection to the larger mission, thereby supporting the clinical supervisor’s potential retention in their work setting.10
Telesupervision expands the opportunity for health professions trainees to be clinically supervised by individuals with the cultural knowledge specific to the patient population served (ie, those individuals working within or knowledgeable about the particular rural setting). This supports higher quality training and patient care, even if the trainee’s primary physical location is not colocated with the clinical supervisor.
Telesupervision can expand the number of clinical supervisors and rotations available within a health care system or clinic, particularly for specialty services (eg, psychological testing, dermatology) that are not otherwise available within specific geographic regions. Thus, telesupervision enables a supervisor with the needed expertise, specialty, or advanced training at one clinic to supervise a trainee located hundreds to thousands of miles away while serving a veteran who may or may not be colocated with either HCP. For example, the supervisor may be located in American Samoa, supervising a trainee physically residing in Hawaii who provides telehealth patient care to a veteran in Saipan. This also enables health care systems serving rural patient populations to bolster their offerings to support future trainee recruitment.
The more trainees increase their connection to caring for rural veterans, the greater the likelihood they will develop knowledge and contribute to these communities after completing their training. Consequently, telesupervision may be fundamental to improving rural population health, contributing to the sustainability of rural health training programs and workforce retention, increasing access to needed health care in geographical areas of shortage, and allowing trainees to receive supervision from those who are most competent in the specific needs of patients living in rural communities.
The evolving landscape of telesupervision and associated opportunities underscores the need to bolster overall clinical supervision practices. Clinical supervision is more than assuming liability, cosigning notes, and ensuring that the standard of care is met. The provision of clinical supervision is a distinct competency separate from the delivery of clinical care. However, only a small portion of those providing clinical supervision have had formal training in supervision and the development of supervision competencies.13,14 Thus, an HCP can be a highly proficient clinician while still being deficient in the skills needed to be a competent clinical supervisor, with a lack of training in supervision skills undermining engagement in effective supervision.15
Research supports the following as essential components of effective clinical supervision: a working alliance between supervisor and supervisee, inclusive of resolution of strains/ruptures, consistent provision of evaluative feedback, consistent supervision meetings, direct observation of clinical work, and opportunities for trainees to see skills modeled through experiential supervision.13 These elements enable investment in the long-term development of the trainee through deep and nuanced feedback provided, the supervisory relationship, access to mentoring, and assistance with articulating case formulations to enable future health care professionals to provide even better care. Engaging in effective supervision requires both the development of supervision competencies and the time allocation needed to uphold these essential elements. Although vital to quality health care, clinical supervision is not consistently reflected in labor mapping or productivity metrics. Consequently, limited dedicated time for supervision (eg, direct observation of trainees’ clinical care, reflection, and preparation to address trainees’ developmental needs) and heavy workloads remain major barriers to effective supervision.14 The continued expansion of technology-assisted supervision highlights the need for HCP duties and associated clinical supervisory skills (whether in person or via telesupervision) to become more integrated into their roles within health care settings.
Upholding effective supervision practices within telesupervision requires thoughtful implementation. Supervisors should engage in direct observation of clinical work in a manner that enables timely correction of trainees and supplemental clinical care as needed, including interventions that assist trainees. In addition, it is essential that the supervisor provides trainees with access to scheduled, ad hoc, and emergent supervision. Furthermore, the supervisor needs to ensure that, regardless of modality, the supervisor can uphold the competency/learning goal development of the trainee (ie, meet learning needs), effectively deliver and receive constructive feedback, and model critical clinical skills relevant to the clinical training area. Of utmost importance, the supervisory oversight and type of supervision required should match the setting to ensure effective supervision.
In some clinical settings, telesupervision may be less appropriate for upholding all elements of effective supervision while matching the needs of the clinical intervention and the trainee. Thus, supervisors need to engage in the supervisory modality that enables them to effectively intervene in clinical care according to the oversight needed. For example, a physical health care intervention may require the supervisor to provide hands-on guidance for a skill or procedure, whereas the dynamics of an inpatient mental health care setting may have patient care interactions that are not fully met by the use of telesupervision, such as complex patients’ needs, acuity, and crisis management. As telesupervision research continues to expand to better understand these applied complexities, there will be an evolving knowledge of the nuances in the application of telesupervision that best capture the benefits of telesupervision without compromising the quality of training and patient care.
CONCLUSIONS
Clinicians working with HCP trainees have the opportunity to use telesupervision to create a dynamic and rich learning environment while maintaining the quality of training and potentially reducing health disparities experienced by rural veterans. With this opportunity also comes the need to recognize clinical supervision as a competency and an essential role of an HCP. In doing so, a thoughtful approach to supervision will enable the powerful tool of telesupervision to be used to its highest potential in a responsible manner that does not overextend its reach.