Perioperative Considerations for Orthopedic Surgery in a Geriatric Population





Background: With more than half of orthopedic surgeries performed on patients aged ≥ 65 years, optimizing perioperative care in this population is essential. Age-related physiologic changes, multimorbidity, and frailty significantly increase surgical risks, including infection, venous thromboembolism, impaired wound healing, delirium, and prolonged recovery. Effective perioperative management strategies are essential to reduce morbidity and improve functional outcomes.
Observations: Using tools such as the Fracture Risk Assessment Tool and the Comprehensive Geriatric Assessment frailty screening aids in identifying high-risk patients and guiding perioperative care. Preoperative strategies focus on controlling comorbidities, such as optimizing glycemic control for patients with diabetes to reduce the risk of postoperative complications. Assessing the mechanism of injury can provide valuable information about underlying conditions. Comprehensive nutritional evaluation is essential for geriatric patients undergoing orthopedic surgery, since malnutrition is common in this population and may impair recovery and increase morbidity. Postoperative management emphasizes early mobilization, delirium prevention, infection control, and anticoagulation management to reduce complications and improve recovery.
Conclusions: Perioperative management of geriatric orthopedic patients requires a proactive, multidisciplinary approach that integrates preoperative risk assessment, intraoperative vigilance, and targeted postoperative care. Identifying and addressing frailty, optimizing nutrition, and implementing structured plans for screening and rehabilitation are essential to reduce complications and enhance recovery.
More than 40 million surgeries are performed annually in the United States, of which > 18 million are orthopedic, including > 1 million emergency orthopedic surgeries and > 2 million joint replacements.1-4 Notably, > 50% of patients undergoing orthopedic surgery are aged ≥ 65 years, a demographic shift driven by longer life expectancies and an increasing number of older adults remaining physically active for extended periods.5 Osteoarthritis, the most common joint disease, affects 10% of men and 18% of women aged > 60 years, often necessitating an orthopedic joint replacement.6 Perioperative morbidity and mortality are 2.9- to 6.7-times higher in older adults compared with younger adults.7 These risks include infection, venous thromboembolism (VTE), pressure ulcers, reduced mobility, and increased mortality. Due to the high incidence of these complications in older surgical patients, special perioperative protocols and considerations are needed when preparing an older patient for surgery. This review aims to establish concrete considerations and guidelines for perioperative management.
METHODOLOGY
A literature review of PubMed, Google Scholar, and IEEE Xplore identified research on perioperative challenges in geriatric orthopedic surgery. Keywords included geriatrics and orthopedic surgery, perioperative care in geriatric populations, and orthopedic perioperative care. Inclusion criteria were strictly defined to ensure relevance to the geriatric population, with studies focusing on patients aged ≥ 65 years. Exclusion criteria were applied to remove studies that did not involve geriatric populations or orthopedic surgeries or that lacked a clear perioperative focus. Studies were analyzed for design, interventions, and outcomes. Special attention was given to identifying common challenges and trends related to perioperative considerations. We developed a narrative report providing a comprehensive overview of the current understanding of perioperative care for geriatric orthopedic patients to offer practical recommendations for clinicians to use in their practice.
RESULTS
Consistent with the narrative review methodology described, the literature search yielded a broad range of publications addressing perioperative considerations in geriatric orthopedic patients. Articles were screened for relevance to patients aged ≥ 65 years undergoing orthopedic surgery and for applicability to perioperative optimization and postoperative outcomes. Given the heterogeneity in study design, population characteristics, and outcome reporting, findings are presented descriptively rather than being quantitatively pooled. Studies not focused on geriatric populations, orthopedic procedures, or perioperative management were excluded. Key themes included multimorbidity and comorbidity optimization, age-related physiologic changes, frailty assessment and fracture risk stratification, nutritional and bone health management, mechanism of injury considerations, prevention of postoperative complications, and the role of multidisciplinary perioperative care.
Unique Physiological Challenges
The aging process induces a range of physiological changes that can increase morbidity and mortality following surgery. One of the most essential elements to surgical recovery is wound healing, as impairments in this process can lead to adverse events, including infection, cosmetic deformity, and wound dehiscence. The general paradigm of aging involves cell senescence resulting in slower or disorganized functional capacity of these cells.8 While wound healing in older individuals was once thought to be defective, recent research has demonstrated that this process is not absent, but delayed.9
Wound healing is a tightly regulated and evolutionarily conserved process that proceeds through 3 main phases: inflammation, proliferation, and remodeling. Re-epithelialization begins with the migration of epithelial cells from hair follicles, sweat glands, or wound margins (depending on wound depth) and is influenced by oxygen levels, moisture, and growth factors.9 Several characteristics of aged skin contribute to the delayed healing process. Aged skin has fewer hair follicles and eccrine sweat glands, as well as decreased follicle thickness.10 This results in fewer proliferating cells for wound healing and lower amounts of sebum production for skin moisture.11 Furthermore, aged fibroblasts are fewer in number and less effective in synthesizing extracellular matrices, resulting in slower and less tensile wound healing.12 Additionally, microvascular changes associated with aging result in disorganized vasculature, which impairs oxygen delivery to the wound bed and diminishes the influx of proinflammatory cells necessary for effective healing.13 These senescent traits of aged skin contribute to the delayed wound healing process found in geriatric patients.
Compounding these age-related factors is the prevalence of multimorbidity, or coexisting chronic diagnoses, in 55% to 98% of older patients.14 Common comorbidities include peripheral arterial disease, chronic venous insufficiency, type 1 and type 2 diabetes, neoplasms, atherosclerotic disease, and hypertension. Older patients are more likely to be prescribed corticosteroids and chemotherapeutic agents that impair the function of inflammatory cells necessary for wound healing.15,16 Additionally, decreased mobility is more common in geriatric patients, which can increase the risk of wound formation, particularly pressure ulcers.17
Perioperative Considerations
All surgical patients undergo a formal or informal preoperative evaluation to assess their fitness for surgery, with the goal of minimizing both anesthesia-related risks and postoperative complications. A widely used tool in this assessment is the American Society of Anesthesiologists (ASA) physical status classification, which stratifies patients into 6 categories based on their medical history and overall health status.18 Classes range from healthy patients (Class I) to organ donors who are brain-dead (Class VI).
Cardiac optimization is an essential component of preoperative evaluation for older adults due to their higher risk of underlying cardiovascular disease.19 This process involves an in-depth review of the patient’s cardiac history, including the timing and nature of any prior interventions and the recurrence rate. Functional capacity is assessed through metabolic equivalents, where a threshold of > 4 metabolic equivalents (the ability to walk up a flight of stairs) is considered adequate for surgery. Risk is assessed based on the specific surgical procedure, and nonemergent orthopedic procedures are considered intermediate risk. If a patient is deemed high risk at any stage of this evaluation, further cardiac testing is indicated.
Pulmonary optimization is typically necessary for geriatric patients, who are more likely to have conditions such as chronic obstructive pulmonary disease or interstitial lung disease.14,20 In patients without severe systemic lung disease, pulmonary optimization involves assessing the functional expiratory volume and diffusing capacity for carbon monoxide. In addition, aggressive modification of risk factors, such as smoking cessation, is strongly recommended.
Additional perioperative conditions are disease-specific and involve evaluation of comorbid illnesses and recognition of absolute contraindications to noncardiac surgery. For instance, an ejection fraction of < 35%, a history of myocardial infarction within 6 months, or active diabetic ketoacidosis are all absolute contraindications to elective surgery. For orthopedic procedures, additional contraindications include symptomatic bacteremia, active joint or local tissue infection, severe malnutrition, uncontrolled metabolic syndrome or chronic disease, untreated immunodeficiency, and active deep venous thrombosis (DVT) or pulmonary embolism.21
Bone Health and Nutrition
In the context of orthopedic surgery, the hallmark of clinically defined optimal bone health is a musculoskeletal system that provides the ability for pain-free functional and occupational tasks with an adequate capacity to withstand the mechanical forces imparted by everyday life. Back pain and arthritis are the fourth- and sixth-most common complaints in primary care, underscoring suboptimal bone health management in developed countries.22
Optimizing bone health through proper nutrition is crucial in the perioperative management of geriatric orthopedic patients. The clinical diagnosis of malnutrition has well-studied associations with worse outcomes after orthopedic surgery, which include increased mortality, hospital length of stay, readmission rates, and health institution spending.23-25 Some studies show that up to 60% of geriatric patients may be malnourished.26
Regarding vitamin and mineral supplements, the general consensus before orthopedic surgery is that vitamins A, C, D, and E, and zinc are predictive in determining postoperative health.27 However, Curtis et al state that therapy should be targeted at correcting relative deficiencies; supraphysiologic concentrations of these vitamins do not appear to be helpful.27 This claim may merit serum studies to rule out deficiencies. Dietitians should be involved in the creation of a patient care plan in the spirit of multidisciplinary orthopedic surgery approaches, which have proven to result in superior patient outcomes.28 Additionally, directive counseling should be provided when necessary.
In patients with adequately managed nutrition, 7 to 10 days of diet optimization is typically sufficient, but patients with malnutrition may require sustained nutritional support for up to 6 weeks; a standardized time for adequate nutrition supplementation has not been identified.25-27 Postoperative management is similar in older patients who are malnourished and those receiving adequate nutrition after orthopedic surgery, which typically involves 3 weeks of a high-protein diet.26
Evaluating Mechanisms of Injury
Assessing the mechanism of injury (MOI) is essential to developing an appropriate and successful orthopedic treatment plan. MOI is typically categorized as low energy, which consists of ground-level falls and other minor trauma, or high energy, which can include motor vehicle crashes or falls from a height.29 Unlike younger patients who typically experience trauma from high-energy MOIs, geriatric patients often sustain fractures from low-energy MOIs. The importance of assessing MOI for the geriatric population is magnified as it provides vital clues that not only help determine the nature of the injury, but also highlight underlying frailty, comorbidities, and potential complications. Weakness or deconditioning related to older age is often not discovered before trauma, which is why assessing the MOI can provide valuable information regarding overall patient health.30
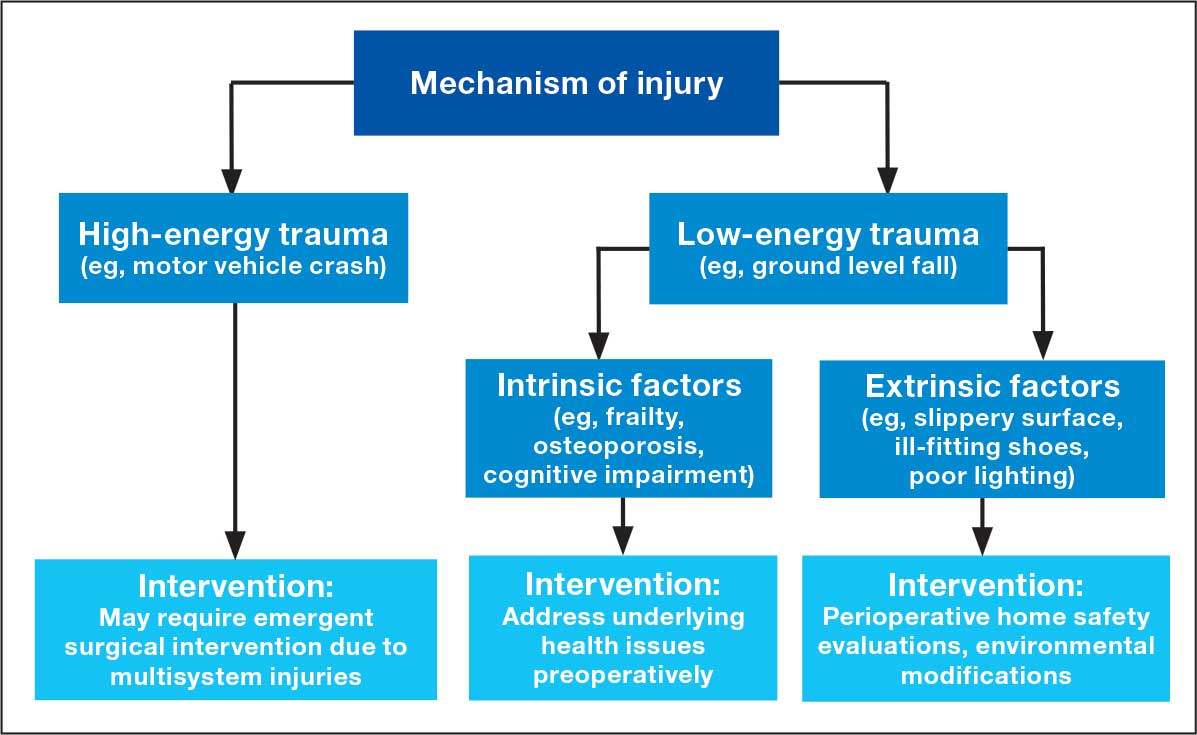
The MOI of trauma also is correlated with factors that influence postoperative recovery and overall prognosis (Figure). Falls comprise more than three-quarters of the MOI in geriatric patients with trauma, and > 90% of these falls are ground-level or other simple falls.30 Falls secondary to an intrinsic disorder, rather than an extrinsic environmental hazard, are more common in geriatric patients.31
These events may be associated with an underlying medical condition, such as osteopenia, osteoporosis, or neuromuscular disorders, such as Parkinson disease.32 They may also be attributed to normal age-related changes, such as decreased visual acuity, reduced reaction time, or mild cognitive impairment.30 An estimated 6% to 35% of geriatric patients who present to the emergency department have some degree of cognitive dysfunction.33 Accordingly, a thorough understanding of the events leading up to injury is vital for the management of older patients. Knowing the specific circumstances of a fall can provide insight into the patient’s gait, balance, and need for further investigations such as cognitive screening or evaluation of home safety. This information can guide decisions regarding preoperative optimization of medications and postoperative rehabilitation interventions.
Frailty and Risk of Fracture
Frailty is a clinical syndrome defined by overall decreased capacity for the body’s adaptive changes to various stressors.34 It is a common condition in geriatric populations due to cumulative degenerative changes and multisystem decline over a lifetime’s worth of disruptions to natural homeostasis.34 In orthopedics, frailty typically refers to musculoskeletal durability and resilience in response to mechanical forces (ie, falls, trauma, and high-acceleration movements). Globally, > 200 million people have osteoporotic frailty, leading to 9 million hip fractures annually.35 More than 30% of people aged ≥ 65 years fall ≥ 1 time per calendar year.36
Assessing frailty in geriatric patients undergoing orthopedic surgery is vital, as it predisposes patients to higher rates of morbidity, mortality, and institutionalization, particularly from falls and resultant fragility fractures.37-39 This is true for a wide range of orthopedic procedures, spanning elective to urgent surgeries and involving the axial and appendicular skeleton.40,41 Given the high rates of fractures, subsequent patient morbidity, and financial burden on the health care system, effective frailty screening is essential.
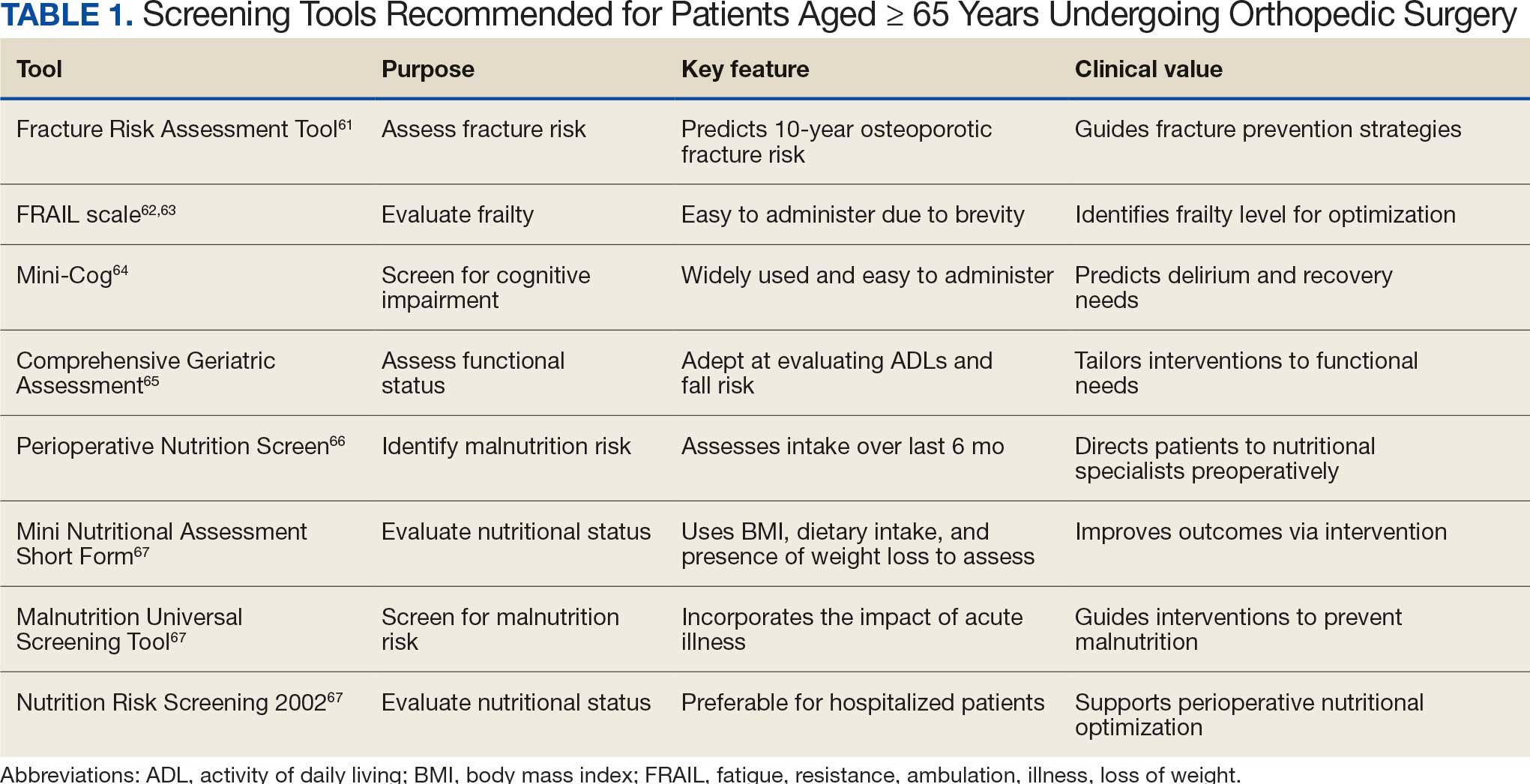
There are many strategies to assess frailty risk and subsequent fracture risk.42 Questionnaires or online medical calculators serve as easy-to-use tools for assessment of frailty or associated predictors of fragility fractures. Validated assessment tools are provided in Table 1.
Dual-emission X-ray absorptiometry is a well-established way to determine bone density and establish fracture risk. The Fried Frailty Phenotype score and Short Performance Physical Battery test are clinically applicable methods of assessing frailty in older outpatient populations. Although these examinations focus on different aspects of the patient, they have moderate agreeability, are sensitive, and can be readily performed in the clinical setting as demonstrated by a > 90% patient participation rate for both methods.42 Finally, several serum studies can be predictive of frailty, the most readily modifiable of which are vitamin D3, ferritin, albumin, and calcium.43 Although they are more invasive for the patient, serum studies can provide additional modifiable targets for perioperative optimization and contribute to risk stratification.
Risk stratification should take place around 6 weeks before surgery, which should provide adequate time for rectification of preoperative barriers to elective surgical intervention—namely nutritional status. In cases of urgent or emergent procedures (ie, femoral neck fracture with concern for avascular necrosis of the femoral head), this may not be possible but should be conducted nonetheless for patient-specific postoperative rehabilitation and risk reduction.
Postoperative Complication Risks
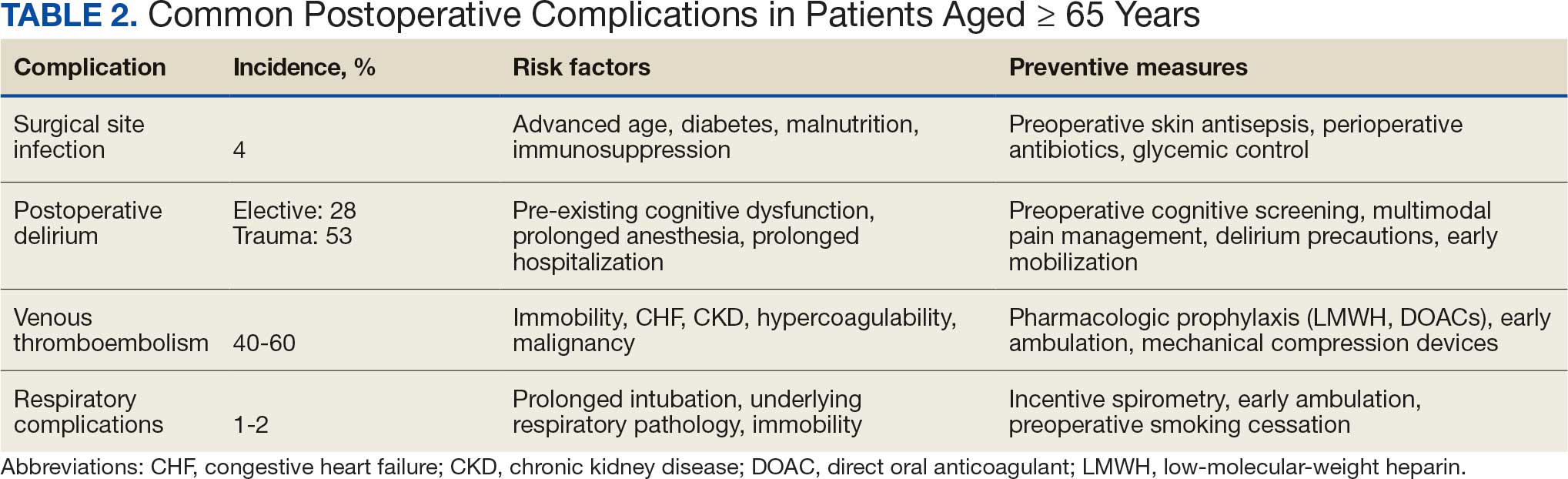
Postoperative complications affect nearly 15% of geriatric orthopedic patients, highlighting the need for comprehensive preoperative evaluations to assess risk factors.44 Age-related physiological changes, frailty, and comorbidities complicate recovery and management (Table 2).
Wound healing is impaired in older individuals due to suboptimal circulation and decreased oxygenation that is secondary to age-related changes, as well as the increased likelihood of comorbid conditions (eg, diabetes).7 Surgical site infections can be particularly malicious in geriatric patients, with a 4% incidence.45,46 Hospitalization can be prolonged by a mean 2 weeks, which increases the risk of hospital-associated delirium and iatrogenic complications.46 Both the mortality rate and costs associated with hospitalization are higher for older patients who develop surgical site infections compared with patients aged < 65 years, underscoring the importance of vigilant monitoring, early detection, and effective preoperative screening to identify and manage modifiable risk factors.47
Postoperative delirium is another common complication of orthopedic surgery in the geriatric population, increasing morbidity and mortality. The incidence is reported to be as high as 53.3% in the trauma setting and 28.3% in the elective setting, indicating a need to assess patient risk preoperatively.48,49 Several factors contribute to the high incidence of delirium, including advanced age, longer surgical durations, intraoperative hypotension and hypercapnia, pre-existing cognitive dysfunction, and postoperative sleep disorders.50
VTE is another common cause of complications following orthopedic surgery. The development of DVT can lead to subsequent pulmonary embolism, which can be fatal. Orthopedic surgery patients are already at higher risk of DVT and VTE than other surgical patients, with an incidence as high as 40% to 60%, though it is frequently asymptomatic.51,52 Geriatric patients may be more likely to have concurrent comorbidities that increase hypercoagulability.53 Congestive heart failure, chronic kidney disease, and cardiovascular disease are all more common in older individuals and can increase the risk of VTE by 2-fold.53 While anticoagulation is the standard of care to prevent VTE after orthopedic surgery, geriatric patients require more careful monitoring due to the higher incidence of bleeding complications. Additionally, early postoperative mobilization is critical to reduce the risk of DVT without significantly increasing pain or causing other adverse events.54
Respiratory complications are common after orthopedic surgery, particularly atelectasis and bronchospasm, which can result from intraoperative mechanical ventilation.55 While these conditions are typically self-limiting, more severe respiratory issues such as pneumonia are a significant concern because they may lead to the need for mechanical ventilation and admission to the intensive care unit (ICU). The more severe complications have an incidence of about 1% to 2% in orthopedic surgery patients.56 Preventive strategies, such as respiratory physiotherapy and guided breathing exercises, are crucial to minimize perioperative pulmonary complications and promote optimal recovery. Addressing these challenges through early intervention is essential to improve outcomes.
Multidisciplinary Perioperative Care
Multidisciplinary care in orthopedic surgery involves collaborative management of patient care by general practitioners, surgeons, anesthesiologists, dietitians, physical and occupational therapists, inpatient health care practitioners (HCPs), and social services. The goal of this form of care is to provide a longitudinal sequence of health-optimization tactics that prepare a patient for surgery and give them the best chance of postoperative recovery.
Given that many aspects of geriatric health play a role in orthopedic postoperative outcomes, there are many preoperative factors to consider. As previously discussed, preoperative evaluation of geriatric patients should include nutritional and fragility screening to determine surgical candidacy and target modifiable risk factors for risk reduction. This screening can be conducted by primary care practitioners and orthopedic surgeons in an outpatient setting. A multidisciplinary approach benefits patients by decreasing time to surgery.35
Several large studies have demonstrated the positive influence of a multidisciplinary approach on patient-oriented outcomes in orthopedic patients. Incorporation of this style of care in contrast to surgeon-led perioperative optimization leads to fewer floor and ICU admissions, shorter lengths of stay, and decreased mortality rates.35,57 These findings are broadly applicable to a wide range of orthopedic surgeries and even surgeries outside of the musculoskeletal system.58,59 In addition, this strategy has demonstrated reduced in-hospital health care costs due to shorter lengths of stay and fewer ICU admissions. Physical and occupational therapy also have irreplaceable roles in outcomes after orthopedic surgeries. They have independently been shown to decrease pain, increase range of motion, and increase functionality in daily life.60 These aspects of recovery are essential for geriatric well-being.
Screening Tools
The World Health Organization FRAX fracture risk assessment tool (www.fraxplus.org/calculation-tool) was developed to identify patients at high risk of fracture and subsequent complications and to guide clinical decision-making regarding pharmacologic interventions.61 FRAX calculates the 10-year probability of fracture based on demographic factors, such as age and body mass index, clinical measures (eg, femoral neck bone mineral density), and risk factors (eg, prior fragility fractures, substance use history, and prolonged glucocorticoid use).61 The online tool is easy to use, making it a valuable resource for assessing fracture risk and determining appropriate treatment strategies.
The fatigue, resistance, ambulation, illnesses, loss of weight (FRAIL) scale assesses frailty in older adults. The scale classifies patients into 3 categories: robust, prefrail, and frail. The frail category is associated with an increased frequency of hip fracture and an elevated ASA class.62 Additionally, the FRAIL scale has demonstrated value in predicting hospital length of stay and the risk of postoperative complications.62 It also has shown utility in quantifying frailty status, which is traditionally challenging to assess systematically.63
The Mini-Cog is commonly used in geriatric populations to screen for cognitive impairment. Preoperative Mini-Cog screening has been shown to predict the development of postoperative complications.64 Geriatric patients who screened positive for cognitive impairment prior to orthopedic surgery were more likely to develop postoperative delirium, require alternative discharge disposition, and have a longer hospital length of stay.64 Mini-Cog serves as an important preoperative tool for identifying patients who may benefit from closer postoperative monitoring and tailored care.
The Comprehensive Geriatric Assessment (CGA) is a multidimensional evaluation that has been validated for use in geriatric patients undergoing orthopedic surgery.65 The CGA assesses functional status and the ability to perform activities of daily living (ADLs), such as eating, dressing, and ambulating. Poor ADLs are associated with increased risk of falls and cardiopulmonary complications. The CGA allows HCPs to identify patients at higher risk of complications and tailor interventions that optimize functional recovery during the perioperative period.
Nutritional screening is another component of preoperative evaluation in older adults undergoing orthopedic surgery. The Perioperative Nutrition Screen is a preoperative phone assessment of unintentional weight loss in the past 6 months.66 Patients who screen positive are asked to come in for a preoperative visit with a registered dietitian who can further evaluate the nutritional status of the patient.
The Mini Nutritional Assessment Short Form (MNA-SF), Malnutrition Universal Screening Tool, and Nutrition Risk Screening 2002 have all been validated for use in older patients undergoing orthopedic surgery. Among these, the MNA-SF has demonstrated superior utility in predicting hospital readmission and mortality.67 Given the established links between malnutrition and poor surgical outcomes, routine nutritional screening is important for identifying geriatric patients who may require preoperative nutritional interventions.
CONCLUSIONS AND RECOMMENDATIONS
Perioperative management of geriatric patients undergoing orthopedic surgery requires an assessment and strategy focused on risk stratification, patient optimization, and mitigation of potential complications and mortality. Due to the complexity and comprehensive nature of an optimal perioperative plan, creating the plan early is essential to ensure adequate time for patient optimization and care coordination.
Nutrition plays a critical role in the success of surgical procedures, and orthopedics is no exception. Extra care should be taken to preoperatively optimize patient bone health before surgical intervention to enhance recovery and reduce the risk of complications. After an appropriate patient history and clinical picture are gathered, screening tools should be used on a case-by-case basis to further characterize comorbid conditions that may contribute to suboptimal outcomes. Additionally, given the proven association between frailty and fracture risk, frailty serves as a readily quantifiable predictor of patient-oriented outcomes. This should be assessed preoperatively with appropriate risk-stratification tools to determine appropriate postoperative measures to prevent morbidity and mortality.
Orthopedic surgery is increasingly common in geriatric patients, who face higher perioperative risks due to age-related physiological changes, multimorbidity, and frailty. Optimizing preoperative assessment and adopting a multidisciplinary approach—integrating surgeons, anesthesiologists, physical therapists, and dietitians—can improve outcomes, reduce complications, and enhance recovery. The successful use of the tools and strategies outlined in this article by primary care should facilitate access to and recovery from orthopedic surgery in the geriatric population.