Study Directly Links Mechanism of Aura to Migraine Pain





Frustration has long plagued researchers who have sought to link the visual auras experienced by some migraineurs with the later onset of headache pain. But now, direct evidence from a new study in rats suggests that auras – presumed to be caused by waves of depression of spontaneous electrical activity that propagate slowly through the occipital lobe of the cortex – can trigger the activation of meningeal nociceptors.
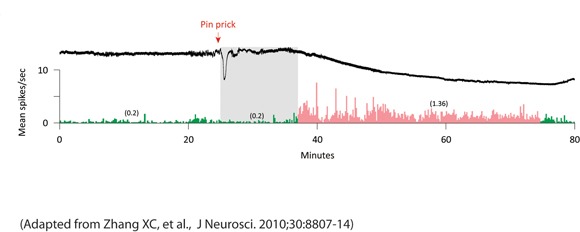
XiChun Zhang, Ph.D., and colleagues at Beth Israel Deaconess Medical Center, Boston, reported that those nociceptors in the trigeminal ganglion of rats became activated either immediately or after an average delay of 14 minutes following the administration of a pin prick, electrical pulses, or potassium chloride to the rats’ visual cortex to induce waves of cortical spreading depression (CSD).
The investigators conducted 83 trials of the three methods of cortical stimulation in 53 rats. Of 64 trials that induced waves of CSD, 31 resulted in increases in neuronal firing rates (25% or greater than baseline) that lasted at least 11 minutes. Sustained neuronal activation was not seen in all but 1 of the 19 trials that failed to produce CSD (J. Neurosci. 2010;30:8807-14).
Long-lasting neuronal activation coincided with the wave of CSD in 10 of the 31 trials in which both waves of CSD and increased neuronal firing were observed.
“The immediate activation of meningeal nociceptors may be clinically relevant to uncommon cases where migraine aura appears together with the headache,” Dr. Zhang and associates wrote.
In the other 21 trials that recorded CSD and increased neuronal firing, long-lasting neuronal activation began a mean of 14 minutes after the CSD waves.
The delayed neuronal activation observed in those 21 trials “may be relevant to the typical delay between the onset of aura and the onset of migraine headache, though the underlying mechanisms remain unknown,” wrote Dr. Zhang and coauthors. They noted that this observation may be the “most clinically promising” because “intervention during the aura phase with drugs that would block the delayed induction of neuronal activation could potentially preempt the onset of migraine headache.”
There were no differences in the pattern of neuronal activation between C- and A-delta-nociceptors or between the methods of cortical stimulation. Responses to cortical stimulation in rats that had their ipsilateral sphenopalatine ganglion excised were no different from those in other rats, which indicated that the parasympathetic innervation of the dura does not contribute to the long-lasting activation of meningeal nociceptors.
The investigators proposed that the sustained activation of meningeal nociceptors could be the result of either a “short-lasting release of algesic molecules” during CSD that promotes an acute activation of the nociceptor and gives rise to an ongoing sensitization that typically outlasts the stimulus by 30-60 minutes, or an ongoing release of algesic molecules for up to 1 hour during CSD.
However, because this period of sustained activation of the meningeal nociceptors may not be sufficient “in and of itself” to explain the 4- to 72-hour duration of the headache phase of migraine, Dr. Zhang and associates proposed that the “duration of nociceptor activation may be sufficient to promote ongoing activity of central trigeminovascular neurons that eventually becomes independent of incoming signals from the nociceptors and can last many hours.”
Dr. Zhang’s research was funded by grants from the National Institutes of Health. Dr. Black has no relevant disclosures.