Pembrolizumab-Induced Bullous Pemphigoid: Navigating Diagnostic Challenges and Treatment Resistance





Immune checkpoint inhibitors (ICIs), including the programmed cell death protein-1 (PD-1) inhibitor pembrolizumab, have revolutionized metastatic urothelial carcinoma management but are frequently associated with cutaneous immune-related adverse events, including drug-induced bullous pemphigoid (DIBP). We present the case of an 81-year-old man with PD-L1–negative metastatic high-grade papillary urothelial carcinoma with a generalized, pruritic, bullous eruption following treatment with pembrolizumab. Histopathology and direct immunofluorescence confirmed bullous pemphigoid (BP). This case underscores the diagnostic challenges of DIBP. Clinicians must maintain a high index of suspicion and consider early transition to steroid-sparing agents such as rituximab in refractory cases. Timely dermatologic referral and close multidisciplinary coordination are essential.
Practice Points
- Suspect bullous pemphigoid (BP) in patients receiving immune checkpoint inhibitors (ICIs) with new-onset pruritus or dermatologic lesions; blisters may be delayed for months.
- Treatment-resistant cases of drug-induced BP warrant consideration of alternative therapies, including rituximab, doxycycline, or intravenous immunoglobulin.
- Multidisciplinary management with dermatology and oncology is essential, as immune-related effects may persist even after ICI discontinuation.
- Encourage patients to report new skin changes promptly to their primary care physician to allow for early intervention.
Bullous pemphigoid (BP) is an autoimmune blistering disorder characterized by the development of tense subepidermal blisters and erosions primarily on the skin, commonly affecting the elderly.1 It is attributed to autoantibodies targeting 2 hemidesmosomal components within the dermoepidermal junction—transmembrane collagen XVII (BP180/BPAG2) and plakin family protein BP230 (BPAG1)—resulting in blister formation due to loss of structural integrity.2 Typically, patients present with pruritic urticarial plaques and tense bullae localized on flexural areas, but cutaneous manifestations vary and can be nonspecific. Histologically, a subepidermal blister with eosinophilic infiltration is characteristic, and detection of circulating autoantibodies against BP180 and BP230 antigens aids in diagnosis.3,4
Drug-induced BP (DIBP) is a subset triggered by medications, including immune checkpoint inhibitors (ICIs) targeting programmed cell death protein-1 (PD-1) or its ligand, programmed death ligand-1 (PD-L1).5,6 Often overexpressed in malignant tumors, PD-L1 inhibits host lymphocytic and apoptotic immune responses. Anti‒PD-1 and anti‒PD-L1 agents, designed to enhance the immune system’s ability to recognize and eliminate cancer cells,7,8 have improved oncologic outcomes for various cancers, including urothelial cancer.9-11 Before 2016, platinum-based chemotherapy was the mainstay for metastatic urothelial cancer management, but US Food and Drug Administration approval of 5 ICIs—nivolumab, pembrolizumab, avelumab, atezolizumab, and durvalumab—transformed treatment options.12Despite robust antitumor responses to ICIs, these medications are increasingly associated with immune-related adverse events (IRAEs), including DIBP, due to inhibition of negative regulators of immunity crucial for maintaining immunologic homeostasis.13,14 Up to 30% to 40% of patients treated with PD-1 inhibitors experience dermatologic complications, such as lichenoid reactions, eczema, vitiligo, and pruritus,15 and patients undergoing treatment with the PD-1 inhibitor pembrolizumab are estimated to be 2.6 times more likely to develop a rash than those receiving standard chemotherapy.16,17 The pathogenesis of DIBP involves autoreactive T-cell activation and subsequent autoantibody production against BP antigens.18 We present the case of DIBP secondary to pembrolizumab immunotherapy in a man with PD-L1–negative metastatic bladder cancer.
Case Report
An 81-year-old man with metastatic urothelial carcinoma presented to dermatology with a pruritic rash characterized by blisters of 5 months’ duration following treatment with pembrolizumab. He had a history of non–muscle invasive urothelial carcinoma and underwent intravesical bacillus Calmette-Guerin treatment. Thirty years later, after surveillance cystoscopies, the patient developed hematuria, which prompted pelvic ultrasonography and cystoscopy that revealed a tumor. Transurethral resection of the bladder tumor confirmed invasive, high-grade papillary urothelial carcinoma with vascular and muscle invasion (clinical stage T2NxMx). Due to elevated creatinine levels, neoadjuvant chemotherapy was contraindicated. Instead, the patient underwent cystoprostatectomy with ureteroileal conduit creation and pelvic lymphadenectomy one month later; final pathology revealed pT2aN0M0 disease with multifocal carcinoma in situ. At that time, there was no evidence of distant metastasis. Surveillance 5 months later identified pulmonary nodules that were confirmed as metastatic urothelial cancer by positron emission tomography/computed tomography (CT). The patient received 6 cycles of paclitaxel (175 mg/m² on day 1) and gemcitabine (1000 mg/m² on days 1 and 8 every 21 days), with progressive disease 16 months later. Despite 0% PD-L1 expression, pembrolizumab 400 mg intravenous (IV) treatment every 6 weeks was initiated 2 months later, and subsequent positron emission tomography/CT showed a positive response at 3 and 7 months after treatment initiation. After the patient’s sixth cycle of pembrolizumab, a generalized maculopapular rash involving approximately 50% of the body surface area led to discontinuation of pembrolizumab, initiation of multiple courses of prednisone and prednisolone, and a dermatology referral.
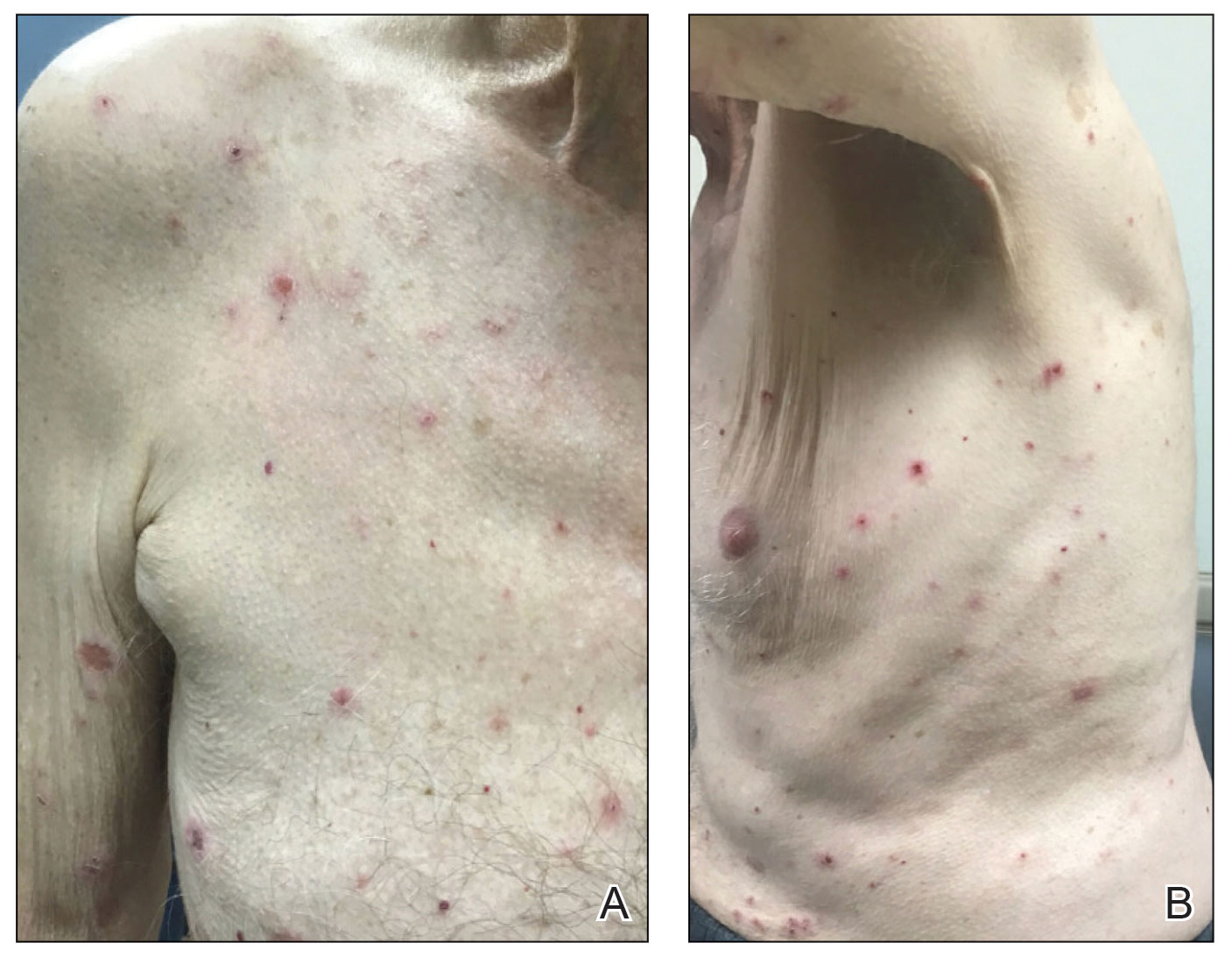
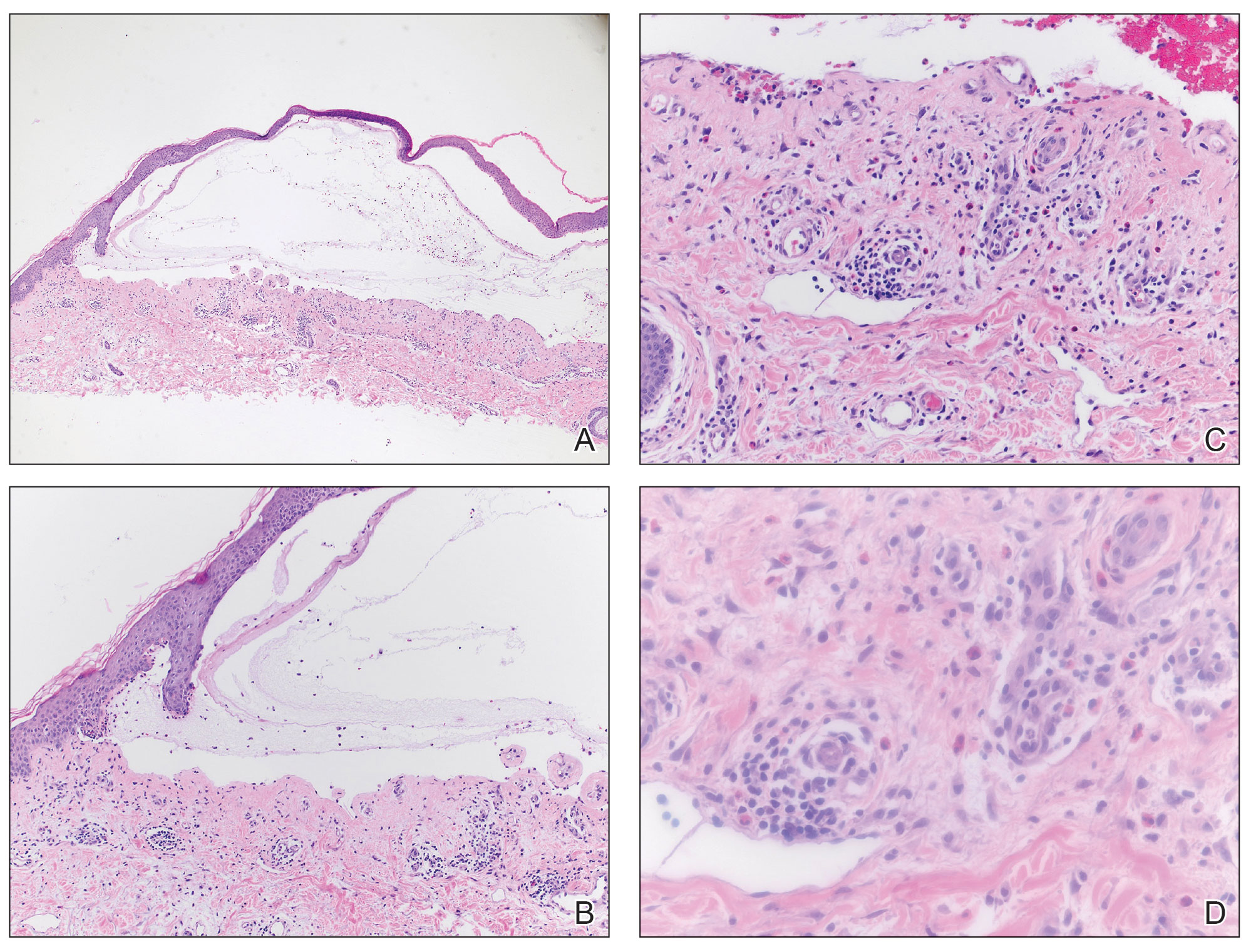
At the current presentation, the patient exhibited excoriated red patches on the abdomen, wrists, arms, upper chest, and legs (Figure 1). Tense blisters were observed on various areas, including the ear and arms. The provisional diagnosis was pembrolizumab-induced BP, supported by the clinical history, presentation, and an initial positive response to steroids. Treatment included topical triamcinolone 0.1% ointment and prednisone 40 mg daily. Biopsies revealed subepidermal blisters with underlying eosinophils on histopathology (Figure 2). Direct immunofluorescence showed strong linear basement membrane zone staining with IgG and C3, consistent with a diagnosis of BP.
One month later, the patient was given the first of two 1-g doses of rituximab, chosen as a treatment due to metastatic cancer history and ongoing severity of the DIBP. In addition, a slow prednisone taper was initiated. Atovaquone 1500 mg daily was ordered for Pneumocystis jirovecii prophylaxis. Following the first rituximab dose, the patient became clear of DIBP but required treatment for a chronic urinary tract infection, delaying the second rituximab dose. The prednisone taper continued, however, and the patient reported re-emergence of several blisters, followed by resolution of pruritus following the second rituximab dose. Bilateral pulmonary embolisms were noted on a restaging CT, attributed to the underlying malignancy and inflammation from DIBP. Doxycycline was initiated at 100 mg twice daily, and prednisone was slowly tapered (as tolerated by the patient’s symptoms) down to 2.5 mg daily approximately 6 months after rituximab initiation. The patient remains in clinical remission at last follow-up; however, considerations for further treatments have included intravenous immunoglobulin.
Comment
This case highlights major clinical challenges in the diagnosis and management of DIBP in a patient with metastatic urothelial carcinoma receiving ICI therapy. Our patient’s clinical course offers several high-yield lessons regarding diagnostic latency, treatment resistance, and a multidisciplinary approach to management.
Pruritus as a Precursor—Since an initial report in 2015, the emergence of DIBP postpembrolizumab has been well described in the literature.19-22 Pruritus is frequently the earliest symptom, preceding bullous eruption. Similar to our case—in which DIBP developed 30 weeks after pembrolizumab initiation—the classic clinical presentation and formation of bullae often are delayed, typically occurring 28 and 39 weeks.
Beyond Corticosteroids to Manage Refractory DIBP—Our patient’s DIBP persisted despite multiple interventions, including pembrolizumab discontinuation, corticosteroid therapy, and rituximab administration. Although cases of DIBP in pembrolizumab-treated metastatic urothelial carcinoma patients have been reported, they did not exhibit similar treatment resistance.23-25 As observed in our patient, immunotherapy discontinuation has been reported in at least 40% of all ICI-mediated cases of BP.14 Subsequent management involves low-dose oral corticosteroids and potent topical corticosteroids; the duration of steroid treatment varies widely, ranging from a few weeks to longer than 12 months, with no standardized approach.26 In cases where ICI withdrawal and corticosteroids fail to produce a complete response, monoclonal antibodies such as rituximab, dupilumab, and omalizumab have been used as alternative treatments, with dupilumab recently receiving US Food and Drug Administration approval for moderate to severe BP.27-31 These biologics selectively inhibit autoantibody formation and the inflammatory cascade, and research has pointed toward them as safe and effective options for refractory BP. Although robust randomized, controlled clinical trials on rituximab for DIBP still are lacking, prospective and retrospective cohort studies have shown promising results, including complete remission rates of 67% to 90%, along with a decline in circulating BP180-specific B lymphocytes, anti-BP180 IgG, and the expression of proinflammatory IL-15 and IL-6.32
Despite receiving 2 doses of rituximab, our patient experienced recurrence of blisters when prednisone was tapered, prompting discussions about alternative tapering timelines and additional therapies such as doxycycline33 or intravenous immunoglobulin,34 which have emerged as steroid-sparing agents for BP following initial steroid therapy.
Systemic Barriers and the Need for Multidisciplinary Care—This case underscores systemic barriers within the health care system that impede prompt diagnosis and management of conditions such as DIBP. The 5-month delay between the patient’s referral to dermatology and the actual consultation, potentially due to shortages of dermatologists, highlights the need for more systematic urgent dermatologic referrals and streamlined diagnostic pathways in suspected cases of IRAEs. Diagnosis requires comprehensive evaluation, including skin biopsy for histopathologic examination and immunofluorescence studies. Ruling out alternative blistering disorders, such as epidermolysis bullosa acquisita, is crucial before confirming a BP diagnosis. Encouraging direct communication between referring physicians and consultants often can expedite the process, as a call from the referring physician can alert the consultant and speed up scheduling. Notably, the patient’s daughter, who was a patient of the dermatologist herself, played a crucial role in advocating for the dermatology referral. Although this should not be necessary, it highlights the pivotal role families can play in ensuring timely access to specialized care for challenging conditions such as BP.
Lastly, the refractory nature of the patient’s condition, coupled with concurrent chronic urinary tract infection and bilateral pulmonary embolisms, emphasizes the necessity of multidisciplinary collaboration among oncology, dermatology, and primary care in managing DIBP. Consulting experts on IRAEs and coordinating with the oncologist were essential for making informed treatment decisions and facilitating the timely exchange of clinical information.
Conclusion
This case underscores the importance of timely recognition and diagnosis of DIBP in patients undergoing ICI therapy but also highlights the need for individualized treatment approaches and multidisciplinary collaboration when managing adverse cutaneous reactions.