Frontline Supervisor Perspectives on Enabling High Reliability and Fostering a Just Culture at the VHA





Background: This quality improvement initiative explored the facilitators and barriers to establishing and sustaining just culture and high reliability practices within the Veterans Health Administration (VHA). We focused on frontline supervisors who play an important role in applying high reliability organization (HRO) principles in their day-to-day operational environments, where competing demands and resource constraints often pose significant challenges.
Methods: A structured questionnaire comprised of open-ended questions was completed by 97 frontline supervisors across a range of VHA facilities, representing varied geographic locations, facility sizes, and levels of complexity. The questionnaire aimed to identify the facilitators and barriers to implementing HRO practices and fostering a just culture within the operational environment. Responses were analyzed using a grounded theory approach, applying open, axial, and thematic coding to identify key themes.
Results: This analysis identified 3 facilitators that supported the establishment of high reliability practices and a just culture: (1) leadership commitment and support, including visible leadership involvement and accountability; (2) open communication and transparency, fostering trust and collaboration among teams; and (3) education and training, which provided supervisors and their teams with the necessary tools and knowledge to effectively integrate HRO principles. Significant barriers were identified, including resistance to change and entrenched attitudes, insufficient resources and funding, and lack of leadership commitment and support.
Conclusions: Our findings provide insights into the experiences of frontline supervisors tasked with implementing HRO principles and fostering just culture within VHA facilities. Leadership support, open communication, and robust training programs emerged as key facilitators, while resistance to change, resource limitations, and leadership inconsistency were significant barriers. These results highlight the need for sustained leadership engagement and resource allocation to bridge the gap between HRO principles, including just culture, and their practical application.
The Veterans Health Administration (VHA) is now in the sixth year of its enterprise-wide transformation into a high reliability organization (HRO). This effort began with a 2016 pilot project and is now implemented in 170 VHA medical centers.1-4 This transformation reflects a commitment to implementing standardized and reliable health care practices.
The VHA HRO implementation strategy includes a multifaceted approach to engage leadership through education, training, leader coaching, and change management initiatives.2 Despite the diversity of facilities in terms of cultures, geographies, and complexities, US Department of Veterans Affairs (VA) medical centers (VAMCs) have increasingly embraced standardized HRO practices. These changes are evident in improvements in VHA All Employee Survey scores, which assess 4 key patient safety culture dimensions: risk identification and just culture, error transparency and mitigation, supervisor communication and trust, and team cohesion and engagement.5 Positive trends in these dimensions highlight a cultural shift toward greater reliability, even amid challenges introduced by the COVID-19 pandemic.
However, this progress has encountered some challenges. Leadership turnover, budgetary constraints, and extensive educational demands for implementing and sustaining HRO practices have created obstacles, particularly for frontline health care practitioners.6 Additionally, there are pockets of resistance similar to what the airline industry faced when implementing crew resource management (CRM). Specifically, senior pilots and legacy leaders were reluctant to abandon their high-status, autocratic management styles and embrace CRM, despite its proven benefits for enhancing commercial airline safety.7 Similarly, some VHA staff have expressed resistance to foundational HRO practices, which include safety huddles, safety forums, leader rounding, and visual management systems.6,8
The training requirements for HRO practices range from a 25-minute introductory course (HRO 101) to a 7.5-hour team training session facilitated by the VHA National Center for Patient Safety (NCPS).9 While some supervisors view these requirements as burdensome, others have demonstrated strong enthusiasm for the process.6 Understanding the perspectives of unit and departmental managers regarding factors that enhance or hinder the adoption of HRO practices is critical for continuous improvement.10-12 Research has suggested that fostering psychological safety can create an environment where new ideas are shared openly, helping organizations navigate resistance to change.13-16
A 2024 quality improvement study, drawing on the perceptions of HRO leads, identified key facilitators, including training, coaching, leader approachability, and psychological safety, as well as barriers such as inadequate training and lack of accountability among managers.17 Building on this work, the current study focused on frontline supervisors, who are directly involved in integrating HRO practices into patient care activities. By addressing both barriers and facilitators, this expanded approach aims to provide a more comprehensive understanding of the challenges influencing HRO implementation in day-to-day operations.
Methods
This quality improvement initiative examined facilitators and barriers to establishing just culture and implementing high reliability practices, focusing on frontline supervisors overseeing clinical care teams (eg, emergency department, critical care) or patient-support functions (eg, dietary services). A questionnaire was sent to a randomized sample of VHA facility supervisors.
A qualitative grounded theory approach was employed to provide a deeper understanding of nuanced phenomena that cannot be captured through numerical data alone. This method enables systematic analysis using open, axial, and thematic coding, ensuring that emerging themes achieve saturation.18,19 It is particularly suited for this study, given the limited prior data on frontline supervisors. Additionally, qualitative methods help mitigate biases common in Likert-style scales, where respondents may lean toward agreement, potentially skewing results.20
Inclusion Criteria
Participants were required to have served as a frontline supervisor for ≥ 6 months. Frontline supervisors are assigned responsibility for supporting staff who deliver services to VHA patients, including clinical care, dietary support, and other functions. These staff must complete baseline HRO cultural training as well as NCPS team training and are responsible for supporting quality, safety, and patient experience. Potential participants were identified from a list of frontline supervisors provided by VHA management. A subset was chosen through random sampling across geographically distributed VHA hospital facilities that vary in size and complexity. Invitations to participate in completing the questionnaire were sent via email, explaining the quality improvement initiative’s purpose, and encouraging voluntary participation. Of 2000 frontline supervisors invited to participate in the initiative, 97 completed the questionnaire. Participants represented a mix of VHA sites in terms of geography, size, and complexity.
Procedures
The authors used a qualitative approach and administered a confidential online survey. Demographic data were collected within the survey to understand characteristics of the participant population, including length of time as a frontline supervisor, facility complexity level, and professional background (clinical vs nonclinical). Survey questions were developed to elicit responses to specific areas of interest based on existing literature related to HRO and just culture.
Facilitators were defined as factors that increase the likelihood of establishing or sustaining high reliability practices and/or culture. Barriers were defined as factors that decrease or inhibit the likelihood of establishing or sustaining high reliability practices and/or culture. The questionnaire consisted of open-ended questions asking frontline supervisors to describe HRO practices and just culture at their individual facility and within their role. Participants also were asked to identify facilitators and barriers that helped or hindered their efforts to establish and maintain high reliability practices and just culture. The questionnaire solicited recommendations for additional support, training, resources, or leadership interventions to strengthen high reliability practices and just culture from each participant.
Analysis
Participant characteristics were analyzed using descriptive statistics. Responses to the 7 open-ended questions were coded and analyzed using ATLAS.ti v.24 qualitative data analysis software by an experienced researcher and coauthor. Grounded theory methodology allowed themes to emerge from the data and although the response rate was limited, the themes reached a saturation point.18,19
Ethical Considerations
Institutional review board (IRB) review and approval were not required for this quality improvement initiative. Formal IRB review and approval of a quality improvement initiative are not required by VHA. Participation was confidential and voluntary, and participants could withdraw at any time without consequences. Completion of the survey indicated consent, and facility names and participant identifiers were not used. Unique numbers were assigned to each participant and all responses were kept confidential and nonattributional. Frequency coding was used to identify the facilitators and barriers to high reliability practices implementation and just culture among frontline supervisors until thematic saturation was obtained.
Results
A total of 2000 frontline supervisors were invited to participate, of whom 97 completed the questionnaire (response rate, 4.9%). Participants were first asked to describe just culture and high reliability practices in their own words. The consensus was that a just culture emphasizes a nonpunitive environment where employees can report errors or incidents without fear of retaliation. It encourages accountability at the systems level, focusing on learning from mistakes to improve processes. In response to a question asking respondents to describe HRO practices and just culture in their own words, participants noted that organizations with a just culture promote open communication, allowing staff to discuss safety issues and concerns without fear of personal blame. Additionally, participants agreed that HRO practices were defined as a set of principles and practices aimed at minimizing errors and promoting safety, especially within complex and high-risk environments. Participants responded that key characteristics include a preoccupation with failure, sensitivity to operations, reluctance to simplify, and a commitment to resilience. HRO practices entail proactively identifying and mitigating risks through open communication and collaboration among team members, they added.
Overall, participants were aligned with their view of the role a frontline supervisor plays in supporting just culture and HRO principles at their facility by fostering open communication and psychological safety, encouraging continuous learning and improvement, and promoting team collaboration and shared accountability. Among frontline supervisors, 93 (96%) identified their role as being critical to creating a safe space and reinforcing just culture and HRO principles at their facility, while 4 (4%) failed to identify a single duty.
Identified Themes
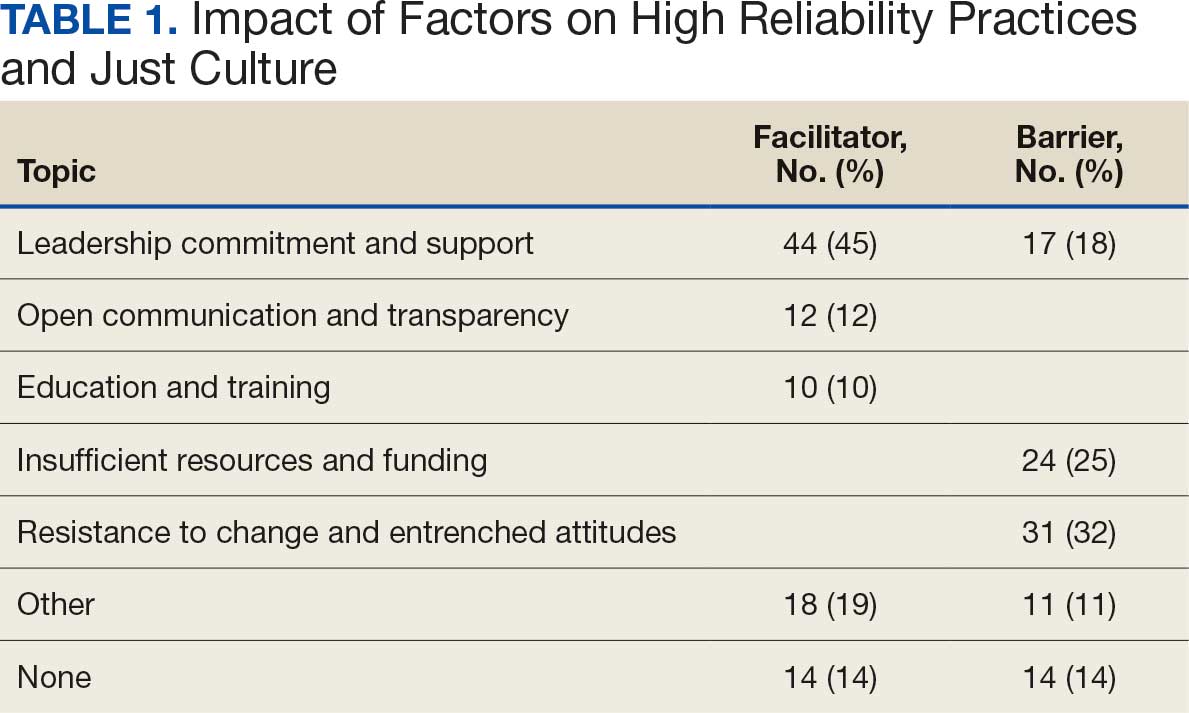
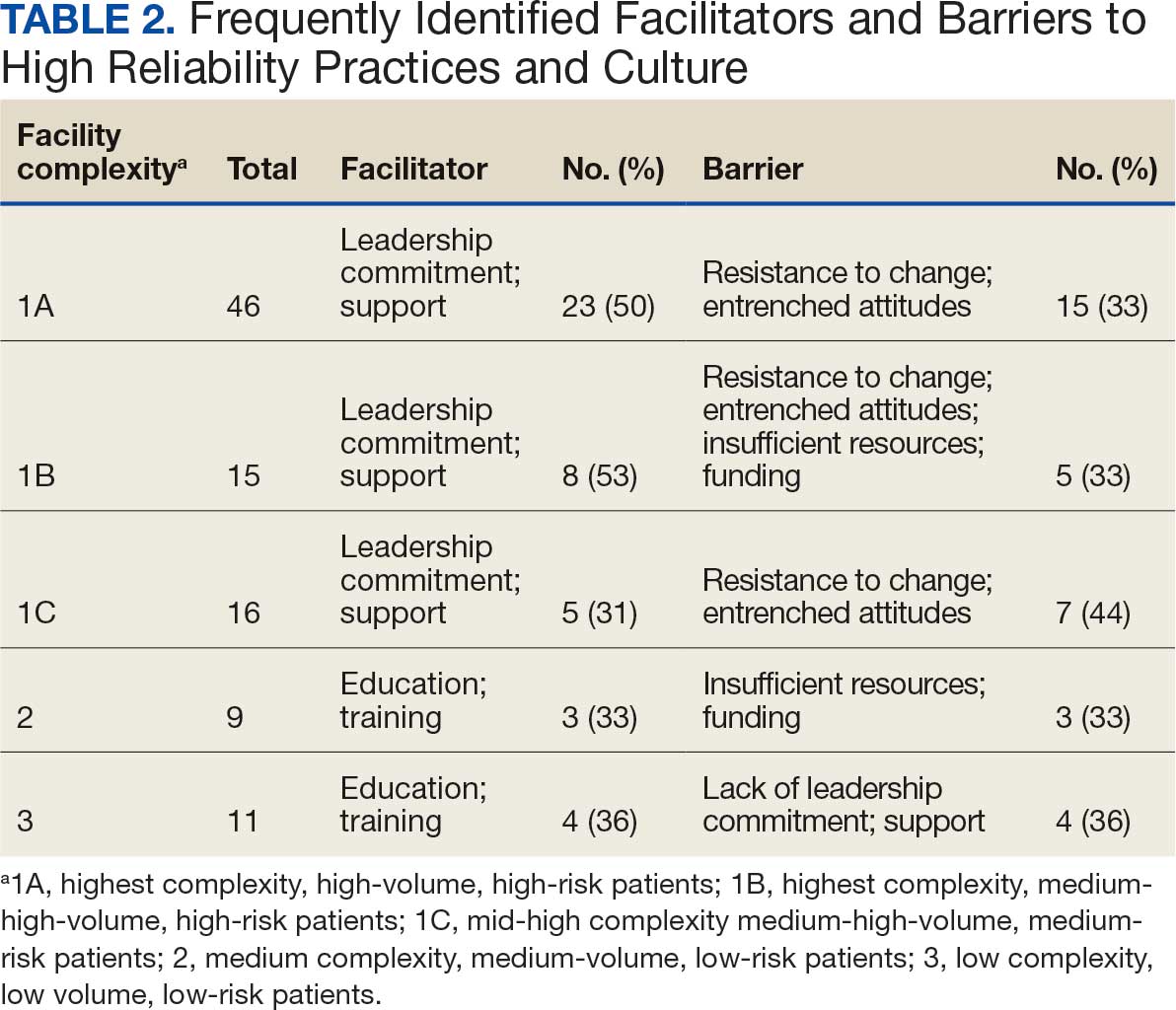
Table 1 summarizes 6 key themes identified from participants’ responses, highlighting the most frequently cited facilitators and barriers to implementing and sustaining high reliability practices and a just culture. Table 2 shows the classification of several themes in relation to facility complexity, emphasizing leadership commitment and support as a pivotal facilitator, while listing resistance to change and entrenched attitudes as a prominent barrier.
Role of Leadership
Facilitators. Leadership commitment and support were the most frequently identified facilitator, accounting for 44 mentions (45%). This aligns with participants’ descriptions of leadership involvement as crucial, particularly in setting standards and fostering accountability throughout the organization. For example, a frontline supervisor with < 5 years of experience from a nonclinical background at a 1B facility remarked, “Facility leadership are involved, which trickles down to lower-level leads and supervisors, which keeps everyone accountable and holds everyone to the same standards.” Participants frequently identified that leaders setting the standard and communicating expectations as paramount facilitators for strengthening high reliability practices and just culture at their facility.
Barriers. A lack of leadership commitment and support was a significant barrier, cited in 17 responses (18%). Participants described this barrier as a deficiency in follow-through, transparency, and presence, which undermines efforts to sustain just culture and high reliability principles. Notably, the lack of leadership commitment and support stood out as a distinct and recurring theme, underscoring its critical role as an independent challenge to achieving organizational goals. “Many leaders are not yet fully bought in,” a respondent explained. “They take the training and pass it off and go right back to their units and focus on blaming or chastis[ing] people for speaking up.” This theme frequently intersected with mentions of insufficient resources and entrenched attitudes, amplifying other challenges.
Open Communication and Transparency
Facilitators. Open communication and transparency were identified as facilitators in 12 responses (12%). Participants emphasized the importance of mechanisms such as HRO meetings and the sharing of “real” examples of positive outcomes from applying HRO principles. Transparent communication fosters psychological safety, allowing staff to report concerns without fear of reprisal. One participant with < 5 years of experience from a clinical background at a 1A facility encapsulated this theme by saying, “Quarterly ‘fireside chats’ are helpful, [this] creates open dialogue about where the next safety issue may occur, what staff need to do their job safely, while also imparting more of the philosophy of HRO that staff may not be aware of.”
Barriers. While communication serves as a facilitator, participants also highlighted barriers such as siloed communication and fear of reprisal. These reflect challenges in creating open and transparent feedback loops essential to high reliability. For example, a participant concluded, “Leadership does not communicate problem-solving efforts and resolution down the chain, they do not see the problems.” Another participant added, “[HRO principles] are not discussed that much.” While this theme presented as a barrier, it was noted less frequently.
Education and Training
Facilitators. Education and training were noted as facilitators in 10 responses (10%), underscoring their role in establishing high reliability practices. Participants suggested tailored training, simulation-based exercises, and mentorship to enhance practical application. However, they noted the importance of linking training to real change and ensuring leadership enforcement of learned behaviors. This theme is best represented by a participant who concluded, “Trainings have helped, but I think as a supervisor, being involved and interacting with your staff, observing, doing the work they do to help identify potential problems areas, especially when new systems are introduced are key. Being hands-on is the only way to successfully manage your team.”
Barriers. Insufficient resources, including time and staffing constraints, were identified as barriers to education and training, accounting for 24 responses (25%). Participants observed that mandatory training without mentorship or application diminishes its effectiveness.
Insufficient Resources and Funding
Barriers. Resource constraints, including low staffing levels and budget cuts, accounted for 24 responses (25%). Participants reported these limitations prevented staff from attending training and affected the overall implementation of just culture and HRO principles. “Low staffing in supporting services as well as in my own service line have created barriers,” a participant reported. Another participant responded that barriers to HRO were primarily “…financial, as the focus is how to curb costs and bring in more funding rather than taking the time to review and apply the concepts of high reliability.”
Resistance to Change and Entrenched Attitudes
Barriers. Resistance to change was the most frequently identified barrier, with 31 responses (32%). One participant described a persistent “gotcha” culture, where blame and punishment hinder progress toward just culture. This entrenched mindset creates significant obstacles to adopting HRO practices and requires active leadership and supervisor intervention to overcome. This theme is best captured by a respondent who noted that “culture change is difficult, especially among staff with such long tenure. It’s a long game.”
Synthesis and Integration of Findings
The data in Table 1 and Table 2 reinforce the themes identified in the qualitative analysis. Leadership commitment and support are pivotal, both as a facilitator and barrier. Open communication and education and training, while recognized as facilitators, were less frequently mentioned, but still critical. Resistance to change and insufficient resources were the most prominent barriers, indicating where organizational efforts should focus to further foster a culture of high reliability.
By addressing these barriers, particularly resistance to change and resource constraints, and leveraging facilitators like leadership engagement and transparent communication, organizations can enhance their implementation of just culture and high reliability practices. These efforts require deliberate strategies, including effective training, mentorship, and the active presence of leadership.
Discussion
This quality improvement initiative builds on prior research by examining the implementation of HRO practices from the perspective of frontline supervisors. Unlike earlier research focused on HRO leads, this study explores the critical role of supervisors who integrate HRO principles into clinical and administrative operations.17 By analyzing their experiences, this study offers practical insights into facilitating HRO implementation across organizational levels.
The findings highlight broad agreement on the value of just culture and HRO principles in fostering safe, accountable health care environments. Participants described just culture as promoting system—level accountability rather than individual blame, encouraging error reporting and learning for continuous improvement. Similarly, HRO practices—emphasizing a preoccupation with failure, operational sensitivity, and resilience— were seen as vital for patient safety in complex settings.
Frontline supervisors play a pivotal role, with 96% of respondents identifying their influence on fostering open communication, psychological safety, and shared accountability. Key facilitators included leadership commitment, open communication, and mentorship. Active leadership involvement was particularly valued, as it trickles down to reinforce standards across all organizational levels. HRO meetings using real-world examples were seen as instrumental in demonstrating the tangible benefits of these principles, helping embed them into daily practices.
Despite these facilitators, several barriers to implementation were noted. Resistance to change and entrenched attitudes, and a persistent gotcha culture undermined efforts to establish just culture. Resource constraints, including staffing shortages and budget limitations, further hindered the adoption of HRO practices. The lack of consistent leadership engagement, marked by limited visibility, follow-through, and transparency, exacerbated these challenges.
HRO leads are important for promoting education and embedding HRO principles into daily operations. These individuals provide vital support to frontline supervisors, translating HRO concepts into actionable practices. However, organizational challenges such as staff turnover and redirected funding have weakened the infrastructure supporting HRO initiatives. The elimination of HRO lead roles due to budgetary pressures at several facilities reflects a short-term focus on operational demands at the expense of long-term cultural transformation.
Additional barriers included siloed communication, fear of reprisal, bureaucratic obstacles, and outdated technology. These challenges limit progress toward high reliability and diminish the effectiveness of HRO principles.
Participants proposed strategies focused on education, training, and leadership engagement. Simulation-based training tailored to specific roles was identified as an effective tool for preparing staff to apply HRO principles in real-world scenarios. Enhanced communication, such as regular leadership rounding and transparent updates on safety concerns, was also emphasized. Participants stressed the importance of showing staff how their feedback influences organizational decisions to build trust and accountability. Finally, standardizing procedures and protocols across facilities was seen as critical for aligning practices and reducing variability in safety processes.
This study underscores the need for sustained leadership commitment and infrastructure to ensure the long-term success of HRO implementation. Addressing the identified barriers and leveraging the proposed mitigation strategies can foster a culture of safety and reliability across the organization.
Limitations
This quality improvement initiative used qualitative grounded theory methods and sampled a relatively small group of experienced leaders specifically involved in implementing HRO within the VHA. In addition, while saturation of themes was reached, the number of responses represents a small sample of VHA frontline supervisors. As such, the findings may not be fully representative of the perspectives of all unit and departmental leaders across the VHA or other health care systems. A previous qualitative quality improvement initiative focused on the perceptions of HRO leads regarding facilitators and barriers to just culture.17 This quality improvement initiative broadened that focus by examining the perspectives of frontline supervisors in the operational environment, who may not be HRO experts but work to implement HRO principles with the guidance of HRO leads (HRO subject matter experts).
There remains an opportunity to address a critical gap by assessing facilitators and barriers beyond the facility level, incorporating both the Veterans Integrated Service Networks (VISN) and VHA Central Office (VHACO). While qualitative methods, such as those used in this study, provide deep insights and detailed understanding, they are limited in their ability to identify system-wide trends and variations at a more strategic VISN and VHACO level. Addressing this could enhance the broader applicability of HRO principles across the VHA.
Conclusions
Successful implementation of the recommendations reported in this study will require sustained focus and continued commitment from all stakeholders across the VHA. As the VHA enters its seventh year on the HRO journey, the risk of organizational drift remains an ongoing concern. Progress has been made, as evidenced by incremental improvements in All Employee Survey scores and increased reporting of adverse events and near misses, but the challenge will be to maintain focus and continue to build upon progress amid the current climate of budgetary constraints.
This study builds on previous quality improvement efforts and provides valuable insights into the barriers and facilitators that can either hinder or support the VHA’s ongoing pursuit of high reliability. The findings offer a model for understanding the complexities of this journey—one that requires continuous effort and adaptation, as there is no definitive endpoint in the quest for high reliability.
Since completion of this study in 2024, the VHA has entered a period of organizational transition and restructuring. Such transitions are often accompanied by increased operational demands and organizational strain. These include realignments, personnel changes, staffing adjustments, workforce reductions, and continued implementation of a new electronic health record system. In this context, maintaining attention to culture, communication, frontline engagement, and mechanisms that provide visibility into organizational climate is essential to sustain momentum in high-reliability efforts.