Cemiplimab for Unresectable Cutaneous Squamous Cell Carcinoma: Experience From a Tertiary Center





The aim of this study was to evaluate outcomes of treatment with cemiplimab in patients with metastatic or locally advanced cutaneous squamous cell carcinoma (cSCC) not amenable to surgery or radiotherapy in a single tertiary center. Demographic, histologic, and clinical data were retrospectively collected for patients treated with cemiplimab between November 2018 and March 2023. The primary objective was overall response rate (ORR), with secondary objectives including progression-free survival (PFS), overall survival (OS), and adverse events (AEs). Among 31 patients, 20 (64.5%) achieved a complete response, 6 (19.4%) achieved a partial response, and 2 (6.5%) experienced disease progression. Our findings yielded an ORR of 83.9%, which exceeded the 46.1% reported in the EMPOWER-CSCC 1 trial. The 2-year OS was 73.5%, comparable to the 73.3% reported in EMPOWER-CSCC 1. Adverse events occurred in 24 patients (77.4%). These findings provide additional real-world evidence supporting the efficacy of cemiplimab in advanced cSCC, with a substantial proportion of patients achieving complete response, including after limited treatment exposure; further studies are needed to better define optimal treatment duration and dosing strategies.
PRACTICE POINTS
- In a cohort of patients with advanced cutaneous squamous cell carcinoma not amenable to surgery or radiotherapy, cemiplimab achieved an 83.9% overall response rate, with 64.5% achieving complete response.
- Two-year overall survival was 73.5%, indicating cemiplimab can provide durable benefit and may improve prognosis in this difficult-to-treat group.
- Adverse events are an ongoing concern; 77.4% of patients experienced adverse events. While cemiplimab is effective, patients taking it need regular monitoring.
Cutaneous squamous cell carcinoma (cSCC) is the second most prevalent skin cancer and ranks sixth in prevalence among all cancers in the United Kingdom.1,2 The etiologic factors underlying cSCC are well established, with major efforts undertaken by governments and public health organizations over the past 2 decades to increase public awareness globally. Known risk factors for cSCC include chronic exposure to UV radiation, radiotherapy, chemical injury, and immunosuppression. The first 3 risk factors amplify risk by increasing accumulation of abnormal gene mutations. Immunosuppression hampers the immune system’s ability to eradicate cells bearing malignant genetic aberrations. Notable gene mutations implicated in cSCC include p53, p16, telomerase reverse transcriptase, NOTCH1, ROS1, mitogen-activated protein kinases, forkhead box M1, and cyclooxygenase 2, in addition to matrix metalloproteinases, which are most commonly associated with Marjolin ulcers.3
The incidence of cSCC continues to surge worldwide,3,4 with more patients presenting with advanced stages of disease and a notable increase in those presenting with unresectable cSCC due to either locally advanced disease or distant metastases.5 Existing therapies for cSCC include surgical excision (including Mohs micrographic surgery); radiotherapy (indicated for cosmetic reasons, locally advanced disease, and/or patient factors); and systemic treatments, encompassing chemotherapy (eg, 5-fluorouracil), and epidermal growth factor receptor inhibitors (indicated locally advanced disease or distant metastases).4
In recent years, immunotherapy has emerged as a potent and effective treatment modality for unresectable cSCC, both locally advanced and metastatic. The success of immunotherapy in cSCC treatment can be attributed to the unique tumor microenvironment of cSCC, which is characterized by high tumor mutational burden, increased density of tumor-infiltrating lymphocytes (TILs), and heightened programmed cell death ligand 1 (PD-L1) expression on neoplastic cells. The elevated TIL density enables a robust immune response, rendering checkpoint inhibitors particularly effective. Greater tumor mutational burden further augments this enhanced TIL activity, amplifying the response to checkpoint inhibitors. Additionally, heightened PD-L1 expression facilitates more effective unmasking by checkpoint inhibitors, thereby enhancing the immune response.6
Cemiplimab is a programmed cell death protein 1/PD-L1 that was approved by the US Food and Drug Administration in September 2018 for treatment of cSCC. It also gained a European Union endorsement in June 2019 and National Institute for Health and Care Excellence approval in August 2019 based on the highly promising results of a phase 2 trial that involved only 59 adult patients with metastatic cSCC.7 The trial reported an overall response rate (ORR) of 47%, durable disease control in 61% of patients, a median time to response of 1.9 months, and response duration exceeding 6 months in 57% of patients. The phase 2 trials reported an estimated 12-month progression-free survival (PFS) of 53% and an estimated 12-month overall survival (OS) of 81%.7
Despite the noteworthy response statistics demonstrated by these studies, it is imperative to recognize that immunotherapies, while potent, are not without challenges. They can precipitate severe immune-related adverse events (AEs), including myocarditis, adrenal failure, and pneumonitis, which can negatively impact patient health outcomes and lead to early treatment cessation. The initial trials reported high-grade AEs such as pneumonitis, pleural effusion, and, notably 11 total deaths, with 8 (72.7%) attributed to disease progression and 3 (27.3%) to AEs.7 Additionally, cost and access to immunotherapy are inherent limitations of the treatment; immunotherapy agents are expensive, and not all centers or patients are able to access them.
The aim of this study was to assess the efficacy of cemiplimab in patients with inoperable cSCC, including locally advanced and metastatic disease, treated at a tertiary referral center in the United Kingdom, and to compare outcomes with the pivotal phase 2 trial that supported regulatory approval of cemiplimab.7 The primary objective was ORR, with secondary objectives including PFS, OS, and AEs.
Methods
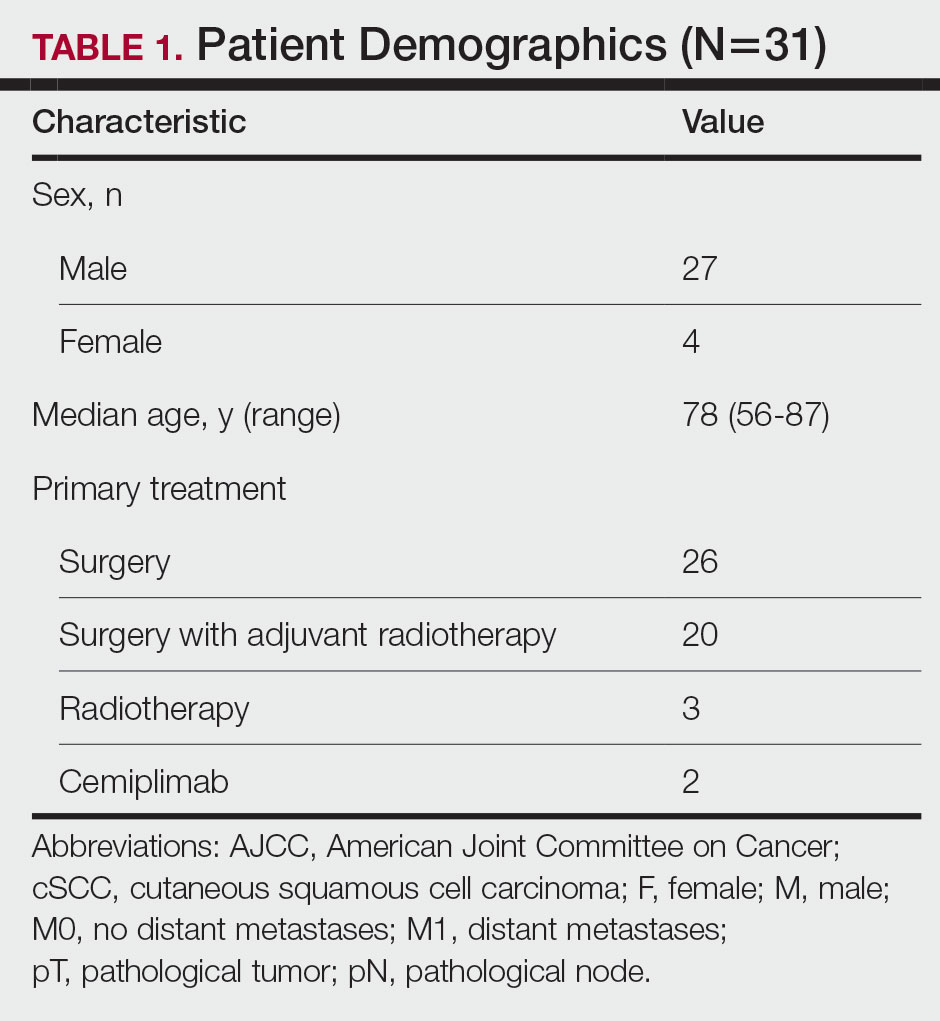
The patients included in this study had unresectable cSCC and therefore were not candidates for surgery or radiotherapy. Patient demographics are presented in Table 1. The main indications for cemiplimab in place of surgery or radiotherapy included local recurrence, locally advanced disease involving deep structures, advanced nodal disease, and distant metastatic disease. Patients meeting these criteria and the following inclusion criteria for cemiplimab treatment from November 2018 through March 2023 at a single tertiary referral center were included in the study:
- Age 18 years or older
- Histologically confirmed cSCC with locoregional recurrence after surgery or radiotherapy, or histologically confirmed advanced or metastatic disease deemed to be inoperable
- Eastern Cooperative Oncology Group performance status of 0 to 2
All enrolled patients received intravenous infusions of cemiplimab 3 times weekly at a dosage of 350 mg. Treatment was continued until complete response, unacceptable toxicity, or disease progression, with a maximum duration of 2 years or 35 cycles. Patients underwent regular follow-up, typically 3 weeks preceding each treatment cycle. Monitoring adhered to the Common Terminology Criteria for Adverse Events, version 4.0, as outlined by the National Cancer Institute.8 Response to treatment was reported according to the guidelines stipulated by the Response Evaluation Criteria in Solid Tumours, version 1.1.9 Written informed consent was obtained for all patients.
Comprehensive patient demographics, histologic profiles, and clinical data were meticulously captured on a retrospective basis. The primary objective centered on elucidating the ORR. Secondary objectives encompassed evaluating PFS, OS, and a comprehensive analysis of AEs. Progression-free survival and OS were calculated by generating Kaplan-Meier curves using Python 3.9 (Python Software Foundation).
Results
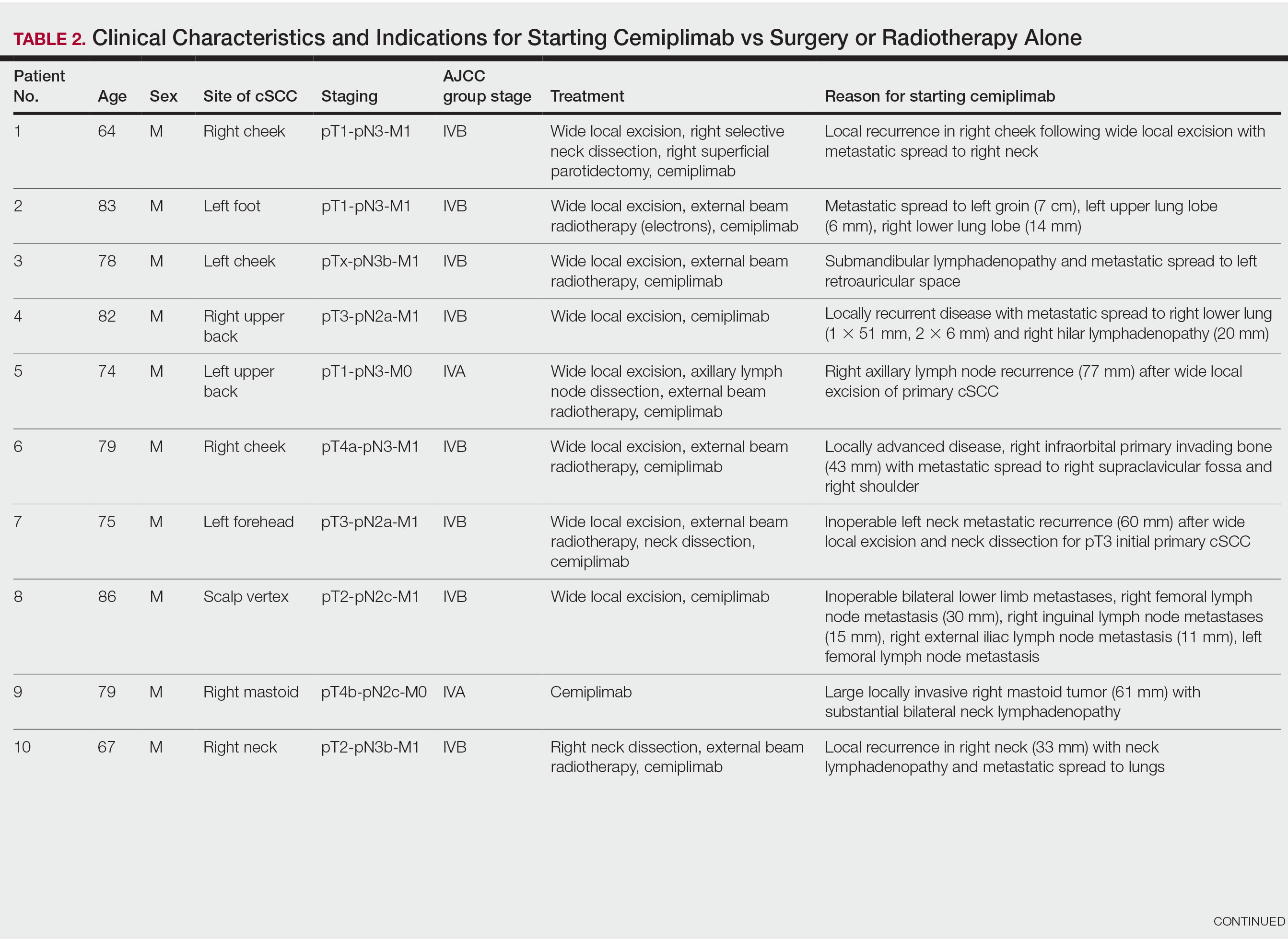
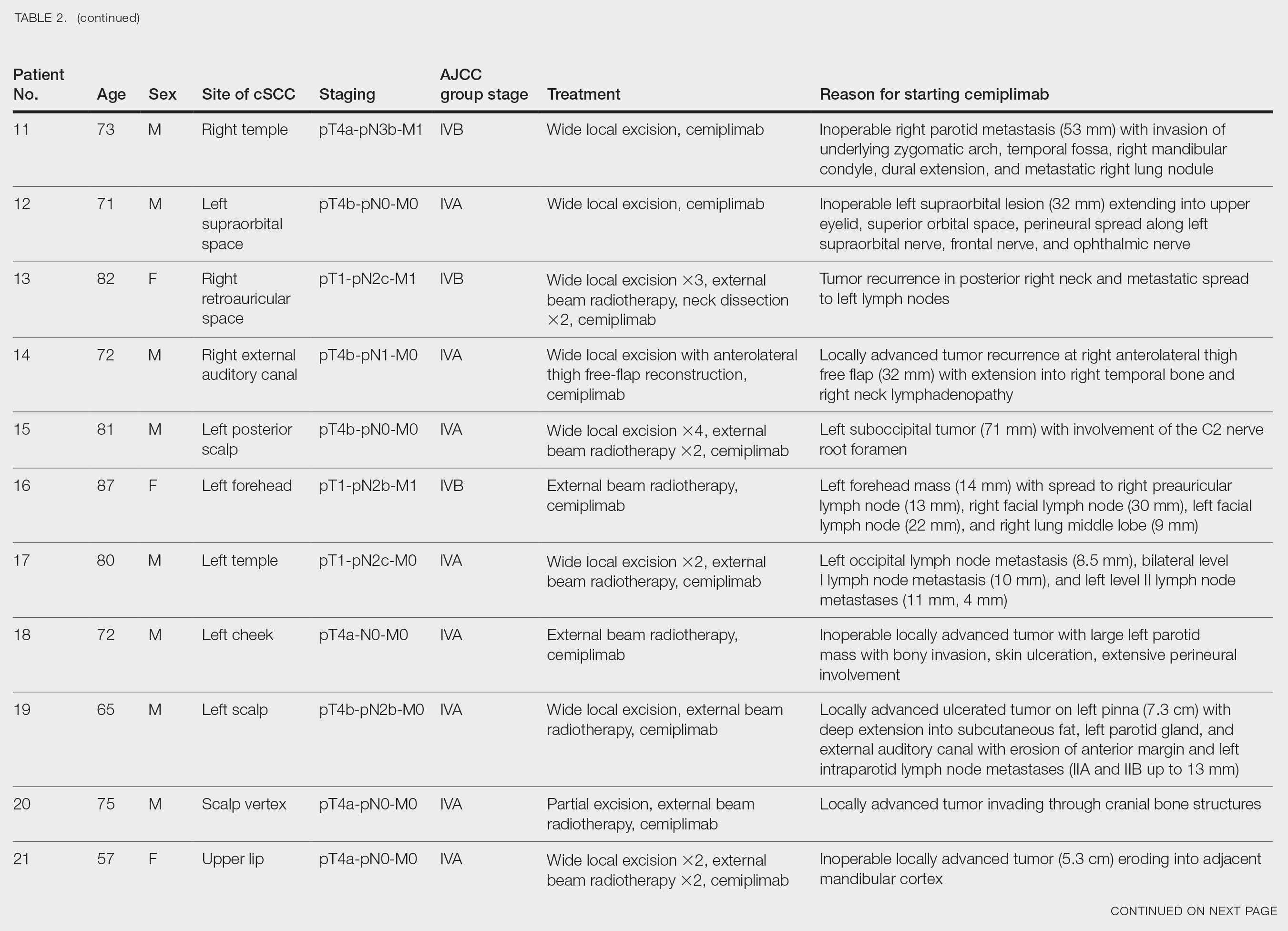
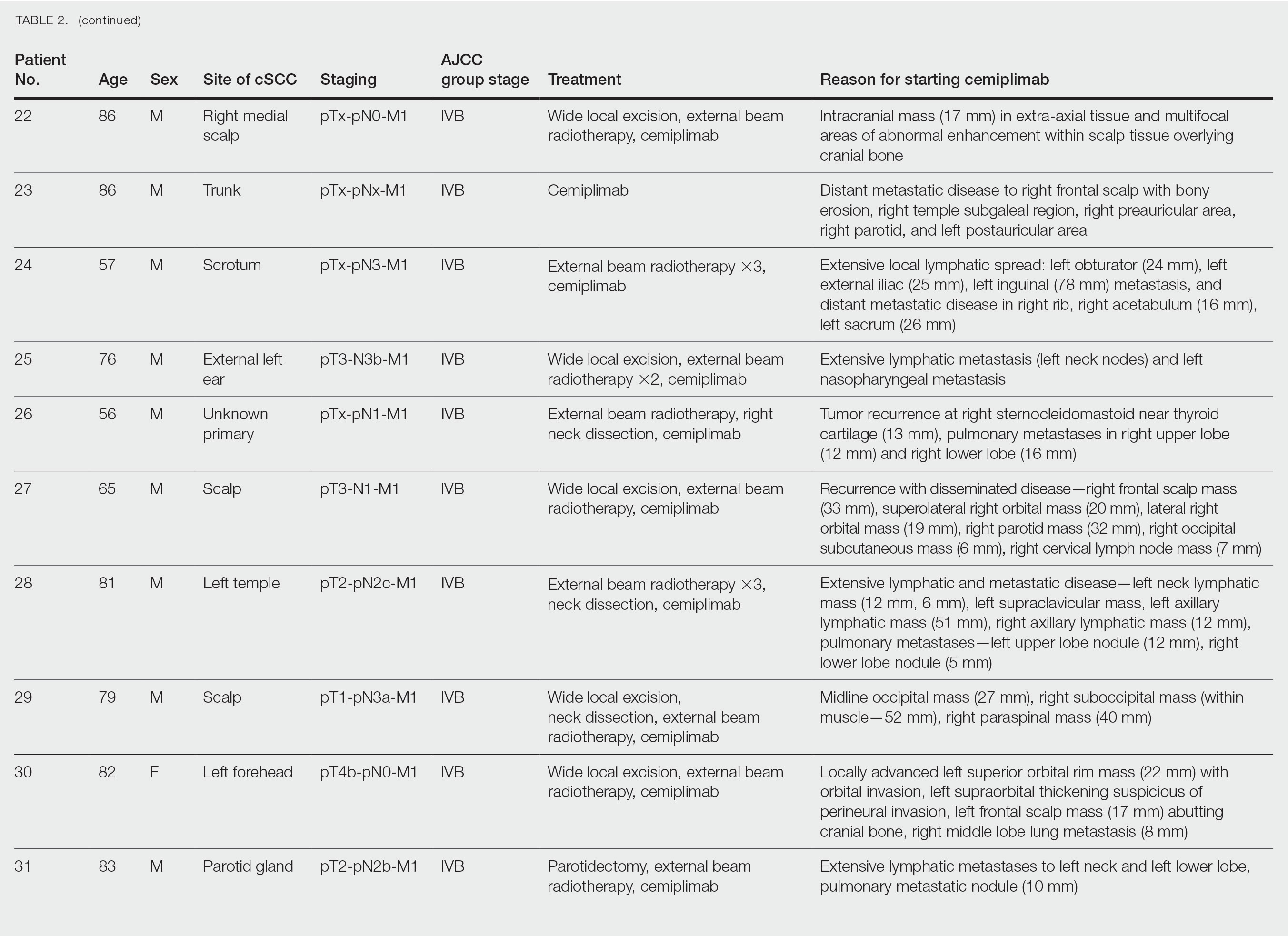
Patient Characteristics—From November 2018 through March 2023, a cohort of 31 patients with inoperable cSCC underwent treatment with cemiplimab at our tertiary referral center. The median duration of follow-up was 13 months. Clinical characteristics are outlined in the Table 2. Four (12.9%) patients successfully completed the full 2-year treatment course. Nine (29.0%) continued to receive cemiplimab therapy at the conclusion of this study in March 2023, with treatment courses ranging from 2 to 11 months since initiation. Ten (32.3%) patients discontinued treatment due to AEs, while 5 (16.1%) regrettably ceased treatment due to mortality. Two (6.5%) patients terminated treatment due to the COVID-19 pandemic, and 1 (3.2%) discontinued treatment as a result of disease progression.
Clinical Efficacy—Of the 31 enrolled patients, a substantial proportion experienced positive clinical outcomes, with 20 (64.5%) achieving complete response and 6 (19.4%) achieving partial response. A total of 26 patients achieved a response on cemiplimab, with an ORR of 83.9% (95% CI, 66.3%-94.6%). Regrettably, 2 (6.5%) patients experienced disease progression, while 3 (9.7%) died before response to cemiplimab could be assessed. Following a median follow-up period of 13 months, the median PFS and OS remained unreached, emphasizing the efficacy of cemiplimab in treating inoperable cSCC (Figures 1 and 2).
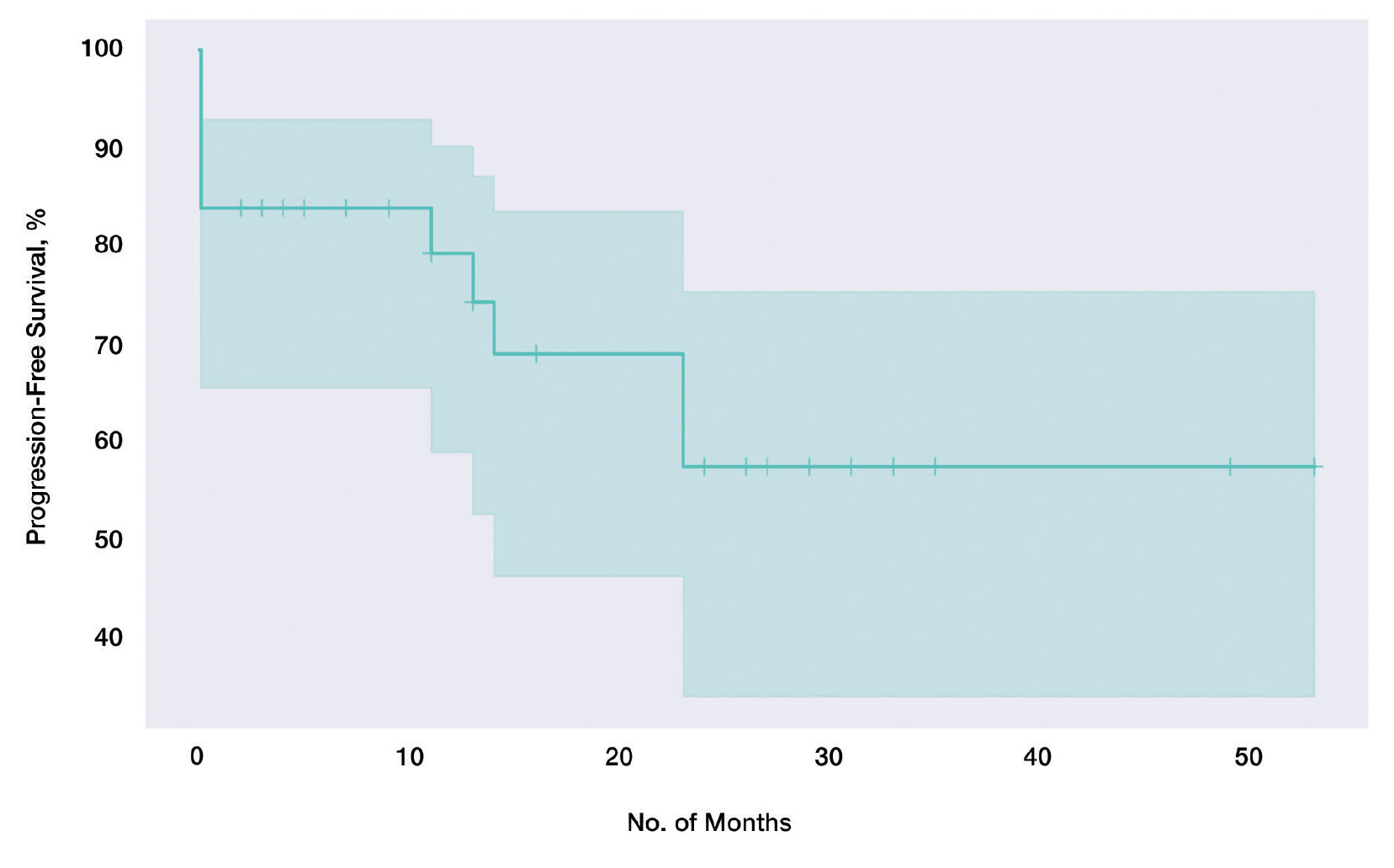
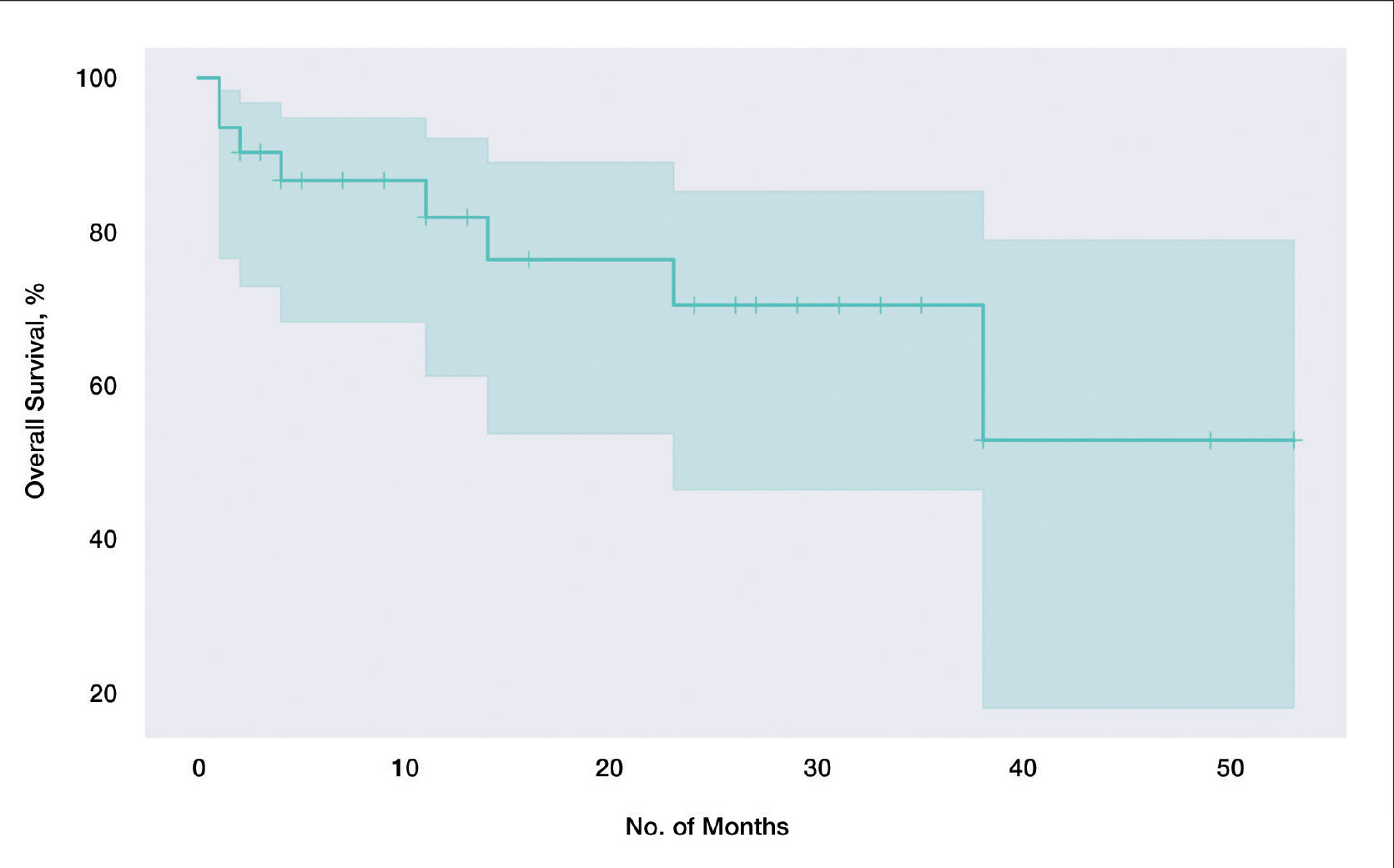
In our cohort, 2-year PFS was 57.5% (95% CI, 33.9%-75.5%) with cemiplimab and 2-year OS was 70.6% (95% CI, 46.5%-85.4%). For PFS, we observed the steepest drops at onset and at the 23-month mark (Figure 1), while for OS we observed the steepest drop at the 38-month mark (Figure 2). Clinically, we observed cemiplimab causing near-complete regression of previously large, ulcerating, fungating cSCC in patients who responded to cemiplimab, mirroring results seen elsewhere.7
Adverse Events and Treatment Cessation—A substantial proportion of patients (24/31 [77.4%]) reported AEs during treatment. Notably, treatment discontinuation was necessary in 10 (32.3%) patients due to a range of AEs, including myocarditis, atrial flutter, pneumonitis, nephritis, derangement of liver function tests, and arthritis. Additional relevant side effects included adrenal insufficiency (3/31 [9.7%]), fatigue (3/31 [9.7%]), diarrhea (2/31 [6.5%]), and type 1 diabetes 1/31 [3.2%]). These outcomes emphasize the importance of vigilance and monitoring when administering cemiplimab in the context of advanced cSCC.
Comment
Historically, advanced cSCC has had a bleak prognosis. The nature of the disease generally meant these patients could not be operated on due to metastatic spread or local invasion, and radiotherapy was not curative. The only option remaining was palliation, but new therapies have shown promise due to specific inherent characteristics of advanced cSCC; for example, the characteristic high mutation burden prevalent in advanced cSCC has paved the way for the emergence of immunotherapy as a promising avenue for intervention.10 Cemiplimab in particular has emerged as a feasible treatment for patients who would otherwise be confined to palliation. Our findings derived from a local cohort reinforce this notion, with a remarkable 83.9% (26/31) exhibiting a favorable response to cemiplimab. Although this local sample of 31 patients is small in absolute terms, in the context of the trial with 59 participants7 that gained global approval for the use of cemiplimab, our study adds a substantial amount of data to the growing body of evidence on the long-term efficacy of cemiplimab. Notably, our results emphasize the potential applicability of cemiplimab among elderly patients and individuals with lower performance statuses: populations historically excluded from immunotherapeutic considerations.
Immunotherapeutic AEs and Tolerance—As anticipated with immunotherapeutic agents, cemiplimab is associated with AEs that also are seen in its counterparts.11 A total of 77.4% (24/31) of our cohort reported immune-related AEs, although the severity warranted treatment discontinuation in only 10 (10/24 [41.7%]) patients, representing less than half of those who encountered side effects and less than a third of the entire cohort. Furthermore, most of these immune-related AEs were managed effectively with short courses of oral steroids, further substantiating the notion that cemiplimab is generally well tolerated across patients of diverse performance statuses. Even for patients who discontinued treatment early due to immune-related side effects, benefits persisted despite the partial course of cemiplimab. Of the 10 patients who discontinued treatment due to immune AEs, 6 (60%) demonstrated stable complete response, 2 (20%) experienced relapse after stopping cemiplimab, and 2 (20%) demonstrated a partial response with stable disease.
Challenges in the Most Vulnerable Patient—Of the 5 recorded mortalities, 2 (40%) were attributed to disease progression, while 3 (60%) occurred before response assessment could be undertaken. The 3 patients who died prior to response evaluation were among the most medically fragile in the cohort, characterized by extensive metastatic cSCC and major comorbidities that, in isolation, posed life-threatening risks. For individuals grappling with widespread metastatic cSCC and substantial life-threatening comorbidities, it is plausible that the necessary physiologic resilience necessary for cemiplimab therapy may be absent. We hypothesize that an immune reconstitution syndrome–like response may be responsible for this early mortality, and these patients may lack the necessary physiological resilience to tolerate this response. This subset of patients warrants careful consideration when considering therapy with cemiplimab.
Conclusion
In summary, our results underscore the efficacy of cemiplimab, as it supported a response in more than three-quarters of our patient cohort. Additionally, the associated AEs, similar to those with other programmed cell death protein 1 inhibitors, generally were manageable with medical intervention. Our findings corroborate earlier studies that have demonstrated the therapeutic potential of cemiplimab in advanced, inoperable cSCC management. In addition to efficacy, our results also suggest that cemiplimab holds promise as a therapeutic option for patients who might not be amenable to the stresses of general anesthesia, surgery, or prolonged hospitalization, although cemiplimab should likely be used with caution in patients with severe, life-threatening medical comorbidities and/or concurrent severe illness. Furthermore, our data demonstrate that the benefits persist not only beyond the completion of the full 2-year course, but also after partial treatment courses discontinued due to patient-specific factors. Future studies would be useful to better understand and optimize dose and duration of cemiplimab treatment to maximize therapeutic effectiveness while minimizing risk of immune-related AEs. Among individuals confronting advanced, inoperable cSCC, cemiplimab is emerging as a viable and beneficial intervention.